The National Association for Trusted Exchange (NATE) and Michigan Health Information Network Shared Services (MiHIN) have released a new video to educate consumers on their rights to access their own health information, and to encourage consumers to take control of their health using smart devices and simple applications to request, view and store their personal health details.
Despite significant efforts from the healthcare industry to improve methods to securely communicate protected patient health data, many consumers remain unaware of their rights and options to view and manage their personal health information. Access to health details can benefit patients in multiple ways, from making it easier to remember health history when filling out forms at a new doctor’s office to helping to care for a family member in need of assistance.
The new NATE/MiHIN video, viewable at http://tinyurl.com/bluebuttonvideo, was created as a brief introduction for consumers and healthcare providers. The video seeks to:
Educate patients and doctors on patients’ rights and options to access their health information
Teach patients how to get a Direct secure email address, which is necessary for secure transmission of health details online
Encourage patients to talk with their doctors about accessing their information electronically
Educate patients on applications enabled with the Blue Button Electronic Health Record Retrieval System for health data
Encourage doctors to adopt Direct secure email solutions to share data with patients
“Using our smart devices with a Blue Button-enabled application enables any of us to receive and share our personal health records using the same secure methods used by doctors today,” said Aaron Seib, NATE CEO. “These Blue Button-enabled applications can help patients make sure their information is accurate, make it easier for you to share your information with all of your doctors, and generally have it available whenever and where ever you need it.”
Guest post by Alex Tate, digital marketing specialist, content strategist and a health IT consultant at CureMD.
Most conductors are sounding out the last call for passengers to climb aboard the ICD-10 train. Although the trains won’t reach full steam until Oct. 1, 2015, the test runs will commence shortly. You’re probably wondering why passengers have to sit through these test runs, right? This is because the journey will last for at least 10 years, so everyone needs to get accustomed to the environment of this locomotive.
Your practice is the train, you are its railroad engineer, the conductor is your practice manager, but who are the passengers? Surely not the patients; they don’t need to apply the codes, do they? The answer to both questions is no. The passengers are your medical billing software vendors, you clearinghouses, your payers, and most importantly – your billers and coders.
If you haven’t started inquiring if these stakeholders and their systems will be ready before time, you could suffer from huge reimbursement disruptions once claims become dependent on these new codes. However, you still have time to get your engines running, and here’s what you need to do:
Contact your medical billing vendor
The first passenger on your train, irrespective of the number of trolleys you’re carrying, is your practice management (PM) or medical billing software vendor. This is because you need to inquire if your billing software is ready for the new codes. If not, you’ll not be able to get your claims through because they’ll contain defunct codes.
Additionally, you must also inquire if the vendor has a clear mapping process for ICD-10 conversion. If upgrades cost extra, or if you’ll need more training, you should have that in mind beforehand.
Lastly, ask them when you’ll be able to begin internal and external testing using these new codes, and if they have any recommendations for streamlining the process.
Those who are familiar with the new Apple smartwatch will know that one of the big focal points for new technology is in healthcare. The “Health Kit” is already available, but now Apple is releasing its “Research Kit.” The information that is collected via their Apple watch Research Kit will be used by scientists and hospitals around the world to understand better a whole array of health issues, such as diabetes, breast cancer and asthma.
Here, The Smart Phone Company provides some insight into the Apple Watch and its development into the Research Kit.
The Key to Medical Developments
The main thing that scientists are lacking, to help them in the understanding of diseases, is numbers. To be able to see patterns and trends, it is useful to have much data to compare, and this is where the Apple watch Research Kit comes into play. By being able to measure a number of variables from people all over the world, scientists and researches can have the information that they need at their fingertips.
With the new Apple watch Research Kit, researchers will be able to design apps which, using existing Apple technology, allows them to gather data that previously was only available in the lab. It also gives Apple watch users the ability to check up on their own health and see correspondences between activity and diet, and their health.
Guest post by Deanne Kasim, IDC research director, payer health IT.
Part of the role of being a research director is to analyze current industry trends, developments and policies and help clients navigate these IT, market, economic and regulatory changes. A post-health reform environment has accelerated the rate of change in all these areas. I recently developed a discussion of the top 10 areas of change payers need to focus on for the next 12 to 18 months (http://www.idc.com/getdoc.jsp?containerId=HI253579). The following is a brief discussion of the top three predictions.
Payers need to develop greater understanding of who their consumers are and adopt more of an omni-channel approach for reaching and meaningfully engaging different population segments.
Consumers understand how to assess the concept of value in other areas of their lives, such as researching information to purchase a new car, a major appliance, or a house. But they do not have nearly as good of an understanding on the way health insurance works, how to necessarily use it, or how to define value in insurance benefits and care choices. Health reform has forever changed the business model of health insurance and placed consumers front and center in the equation. This increased emphasis on the consumer needed to happen a long time ago and now payers are challenged to radically change how they develop, market, and administer health insurance benefits accordingly. IT tools and applications are quickly evolving to better support the consumer’s purchase decisions and use of insurance benefits, and payers are continuing to realize the potential and importance of this developing product area.
According to IDC Health Insights’ 2014 Payer Survey, payers were split between increasing the 2014 budget for consumer engagement strategies (49 percent) and keeping the budget the same (51 percent). I fully anticipate these numbers will be higher in this year’s survey, as more payers commit additional resources to the development and support of thoughtful consumer engagement strategies, processes and IT applications.
As the industry moves from pay-for-volume to pay-for-value payers need to form more “win-win” relationships with providers and this requires leadership, trust and the IT applications and analytics to support this.
The longtime practice of paying for volume is changing rapidly to pay for value, and the U.S. Centers for Medicare & Medicaid Services (CMS) continues to lead developments in pay for value methods, including a variety of value-based reimbursement (VBR) practices, pay-for-performance (P4P) and global or episodic payments. The establishment of patient centered medical home (PCMH) and accountable care organization (ACO) models, combined with the reduced reimbursement realities under the ACA, has incentivized more providers and payers to explore new, mutually beneficial reimbursement arrangements. Providers and payers will have an increasing need for analytics applications to help predict and monitor clinical quality outcomes and financial performance measures in order to make VBR arrangements work for all involved stakeholders. In addition, as payers continue to employ narrow networks as part of their public HIX business line strategy, VBR arrangements with the contracted providers can enhance the performance of both payers and participating providers.
Dean Stephens is the CEO of Healthline, a media group and a health information technology company. Here Stephens discusses healthcare analytics and how it’s important to providers and patients; the ever-increasing importance of harvesting useable and life-changing information from unstructured big data; analytics in population health; the importance of ACOs and the future of Healthline.
Tell me about your background and your role at Healthline. I grew up in a small, blue-collar town in New England and was fortunate enough to attend an Ivy League college, which was a rare thing for this town. After college and graduate school, I got lucky to land a policy analyst position for the Washington State governor, but in no time, got drafted into management consulting at Deloitte. Much of my consulting time was spent in the healthcare industry learning first-hand how “upside down” the industry was. Thus, I joined other entrepreneurs to re-imagine this muddled industry and joined Healthline as CEO in 2001, not knowing then that I would end up building two companies simultaneously.
What does Healthline do and how has the company evolved?
Healthline’s mission is to make the people of the world healthier through the power of information. And we do this through two business units – our media group, which consists of our consumer health website Healthline.com, and our health information technology group, which includes a range of search and data analytics solutions built on our market-leading medical taxonomy. We are currently working with some of healthcare’s largest brands, including AARP, Aetna, Pfizer, Sanofi, UnitedHealth Group, Microsoft, IBM, GE and Elsevier.
Describe your personal view of analytics and what that means to the rest of us. Why is this important?
Healthcare is the most information-intensive industry on the planet. The number of diseases recognized today and the permutations on the treatment matches to individuals have exploded over the past 20 years. It’s impossible for an individual physician or a large, sophisticated provider or payer institution to deliver effective treatment across all patients without analyzing vast amounts of complicated data. We limped along in the traditional fee-for-service realm. Now as the healthcare market shifts to value-based reimbursement, the value of information and analysis rises dramatically as providers shift from being rewarded for sick care to well care.
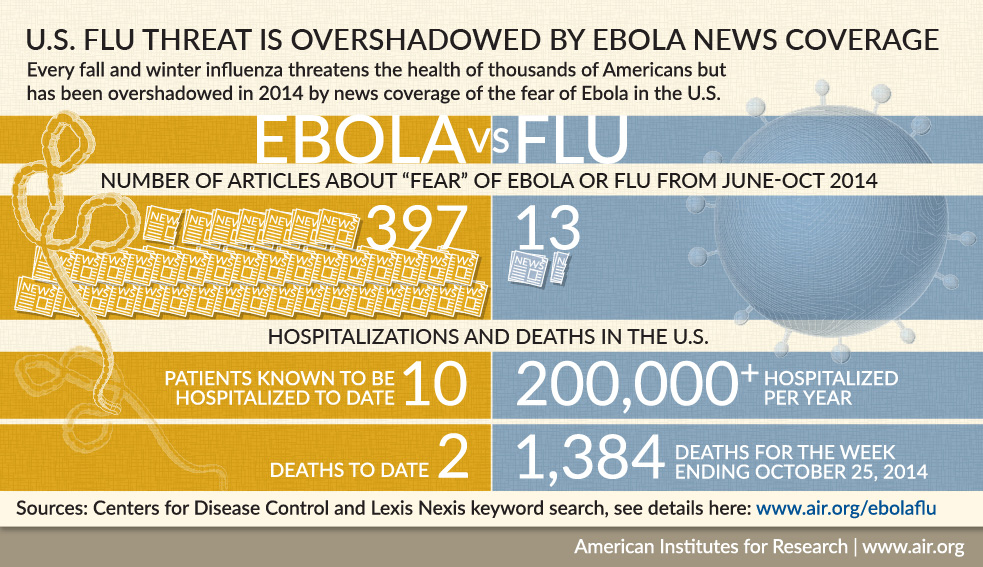
Two big communicable disease scares—Ebola and measles—gripped the attention of the general public recently. They did so with enough strength that the average person on the street spoke out and demanded that actions be taken to protect themselves and families. It was virulent on social media. The total count of Ebola deaths at the end of last year was 5,021 worldwide. The CDC reported 10 Ebola cases treated in the U.S. and two patients died as of January 2015. There were 121 total measles cases in the U.S. this year in 17 states. All but 18 of the measles cases were because of an outbreak that spread from Disneyland in California.
What is remarkable is that these two infectious diseases affected a total of less than 200 people across the nation. Yet it triggered a vigorous response from masses of people who were afraid that they could contract Ebola when the actual chances were significantly lower than dying from a lightening strike. The spread of measles among children erupted into online wars between the vaccinated and unvaccinated.
Contrast this with the lack of concern over the flu vaccine’s low effectiveness against this year’s virus, which the CDC estimates kill 3,300 to 49,000 people in the U.S. every year. Warnings from the CDC that the flu strain this year is worse and getting the flu shot will at least temper the illness seems to have had little effect on increasing vaccinations.
Ebola attracted the public’s attention with such obsessive coverage that the public expected exposed individuals to be quarantined even though an individual had no symptoms to indicate a contagious state. More importantly, contact with fluids of an infected person is necessary to become infected. Contrast this with measles where the air and surfaces an infected person has coughed or sneezed remain contaminated for up to two hours. Measles is contagious up to four days before the telltale rash appears. According to the CDC, about one in every 1,000 children who contract measles will die and 90 percent of the non-immune people close to an infected person will get it.
Fear was the driver for Ebola’s patient engagement. The measles outbreak engaged parents because it raised the issue of the high rate of non-immunized children of a highly contagious and serious disease, but there were no calls to quarantine measles victims and guard them as with Ebola victims.
On Apr. 23, 2015, the Centers for Medicare & Medicaid Services (CMS) issued a proposed rule outlining proposed fiscal year (FY) 2016 Medicare payment policies and rates for the Inpatient Rehabilitation Facility Prospective Payment System (IRF PPS) and the IRF Quality Reporting Program (IRF QRP). The FY 2016 proposals are summarized below.
Proposed Changes to IRF payment policies and rates:
Changes to the payment rates under the IRF PPS. CMS is proposing to update the IRF PPS payments for FY 2016 to reflect an estimated 1.9 percent increase factor (reflecting a new IRF-specific market basket estimate of 2.7 percent, reduced by a 0.6 percentage point multi-factor productivity adjustment and a 0.2 percentage point reduction required by law). CMS is proposing that if more recent data are subsequently available (for example, a more recent estimate of the market basket or multi-factor productivity adjustment) such data would be used to determine the FY 2016 update in the final rule. An additional 0.2 percent decrease to aggregate payments because of updating the outlier threshold results in an overall update of 1.7 percent (or $130 million), relative to payments in FY 2015.
No changes to the facility-level adjustments. As stated in the FY 2015 IRF PPS final rule (79 FR 45872, 45882 through 45883), CMS froze the facility-level adjustment factors at the FY 2014 levels for FY 2015 and all subsequent years, unless and until we propose to update them again through future notice and comment rulemaking. For FY 2016, CMS will continue to hold the facility-level adjustment factors at the FY 2014 levels as we continue to monitor the most current IRF claims data available to assess the effects of the FY 2014 changes.
ICD-10-CM Conversion. In the FY 2015 IRF PPS final rule (79 FR 45872), CMS finalized conversions from the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) to the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) for the IRF PPS, which will be effective when ICD-10-CM becomes the required medical data code set for use on Medicare claims and IRF?PAI submissions. CMS reminds providers of IRF services that the implementation date for ICD-10-CM is Oct. 1, 2015.
The 2013 report found that there was an increase in participation from eligible professionals and in reporting clinical quality information for both PQRS and the e-prescribing Incentive Program, reflecting both increased use of electronic prescribing as well as increased tracking and reporting of important quality information. The report also indicates progress in CMS’ efforts to improve quality measurements, and to encourage building a national electronic health information infrastructure in the United States.
Report highlights include:
Participation in the PQRS program increased by 47 percent from 2012 to 2013.
In 2013, 641,654 eligible professionals participated either as individuals or as part of PQRS group practices, through at least one reporting mechanism, a 47 percent increase from the 435,931 who participated in 2012. Approximately 51 percent of the 1.25 million professionals who were eligible to participate in 2013 participated in PQRS. The 2013 PQRS incentive payments totaled $214,551,741.
469,755 eligible professionals were subject to a 2015 PQRS negative payment adjustment. Based on 2013 PQRS reporting, 469,755 eligible professionals are subject to a reduction of 1.5 percent of their 2015 Part B Medicare Physician Fee Schedule allowed charges. Of those professionals subject to the adjustment, 98 percent did not attempt to participate in PQRS. In addition, 43 percent of the professionals subject to the payment adjustment treat 25 or fewer Medicare beneficiaries a year.

 Those who are familiar with the new Apple smartwatch will know that one of the big focal points for new technology is in healthcare. The “Health Kit” is already available, but now Apple is releasing its “Research Kit.” The information that is collected via their Apple watch Research Kit will be used by scientists and hospitals around the world to understand better a whole array of health issues, such as diabetes, breast cancer and asthma.
Those who are familiar with the new Apple smartwatch will know that one of the big focal points for new technology is in healthcare. The “Health Kit” is already available, but now Apple is releasing its “Research Kit.” The information that is collected via their Apple watch Research Kit will be used by scientists and hospitals around the world to understand better a whole array of health issues, such as diabetes, breast cancer and asthma.