Healthcare is home to some of the most mind-blowing technological advances when it comes to diagnostics and therapies. At the same time, the healthcare system is responsible for many of the most head-scratching operational difficulties related to standard IT processes, such as those involved with moving data from one system or site to another. The same industry that successfully deploys remote-controlled surgery robots to heal a patient also struggles to send a discharge summary to a physical therapist for the same patient.
How can we explain this apparent paradox?
A Model of Interoperability
The simple answer is that interoperability in healthcare is a journey, not a destination. The question “why haven’t we solved interoperability?” assumes that interoperability is a one-time problem, when in fact the systems, standards, and data flows that constitute interoperability are constantly changing as the underlying patterns of treatment and reimbursement change.
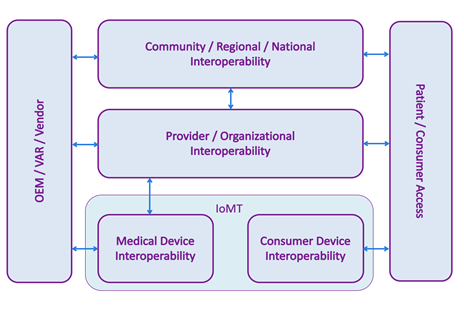
Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine[1].
In the center, provider, or organizational, interoperability indicates data flows within a single organization, typically a hospital or hospital system. This has historically been dominated by HL7 v2 transmitted over a TCP connection on a private network, although other standards and technologies are also used.
At the top, community, regional, and national cross-organizational Interoperability refers to communication of healthcare data across different organizations, for example ACOs, HIEs, and provider-to-payer data flows. In this part of the model, we often see IHE style integrations that exchange entire patient records in a single, secure transaction over a public network.
At the bottom, the Internet of Medical Things (IoMT) is divided into two parts: medical device interoperability, which concerns devices used in a clinical setting, and consumer device interoperability – commercially available devices marketed directly to consumers, such as fitness devices and in-home monitors.
On the left, healthcare IT vendors need to enable their products to interoperate at different levels of the interoperability model, depending on which markets they serve. For example, an EHR vendor will need its product to send and receive HL7 v2 messages in order to participate in the organizational interoperability space.
On the right, we are seeing an increased demand for patient or consumer access to their data, whether it is from a fitness device, a hospital’s EHR, or a payer’s disease management system. Integration in this box is often accomplished using APIs, including FHIR.
Kareo, a provider of cloud-based clinical and business management software for independent medical practices and medical billing companies, announced the sale of its revenue cycle management (RCM) services business unit to an independent supplier of outsourced medical billing services, Health Prime International.
Kareo will now fulfill the growing demand for outsourced medical billing services exclusively through its leading network of over 1,500 medical billing company partners. This shift in strategy enables Kareo to increase its focus on building the industry’s leading cloud-based software platform for independent medical practices and the billing companies that serve them.
“The sale of Kareo Managed Billing will enable Kareo to focus on more quickly advancing our software platform and customer support offerings to continue building on our position as the leading cloud-based software supplier to independent medical practices and billing companies,” said Dan Rodrigues, founder and CEO of Kareo. “We believe this shift in strategy will also help Kareo build stronger relationships with medical billing companies, who in the past were concerned about competing with their software supplier.”
“Once again, Kareo has demonstrated their commitment to medical practices and the billing company industry by focusing their intellect and energies on providing a premier platform for us to use to better support our providers and build their practices. We applaud Kareo for exiting the services side of the business and helping us to grow ours,” said Tracy L. Freeze, president of HMS Midwest, LLC.
Kareo is the first medical practice software company to acknowledge that independent medical billing companies are best positioned to meet the outsourced billing services needs of medical practices. Independent medical billing companies have demonstrated their ability to deliver highly targeted expertise around medical specialty-focused billing, improved reimbursements and increased operational efficiency.
“We’re pleased that Kareo’s decision to sell their RCM services business will give them even more focus and resources to commit to their industry-leading software platform, which gives their billing company partners such a powerful, competitive advantage in the market,” said Ray Shammo, president of PhysicianDS.
Wolters Kluwer, Health released new data from a survey of nearly 2,000 consumers, hospital executives, doctors and nurses in the U.S. on attitudes surrounding breakdowns in care, how costs shape care decisions and the influence of a broad lack of transparency within the healthcare system. Findings from the report, “Mending Healthcare in America 2020: Consumers & Cost,” showed alignment and deep divisions in how patients and providers view healthcare.
Diana Nole
“Leading up to the 2020 presidential election, there has been a shift in attitudes surrounding out of control healthcare costs and a complicated and opaque healthcare system that erodes the trust of consumers and providers. Our national survey echoes this dissatisfaction, but also illuminates that those on the front lines of delivering care are taking diverging, and sometimes conflicting, paths to mitigate their concerns and prioritize actions,” said Diana Nole, CEO of Wolters Kluwer, Health.
“Mending Healthcare in America 2020” examines where each stakeholder observes breakdowns, inconsistencies and a lack of transparency throughout the system and, subsequently, how they make care choices around those perceptions.
Key survey findings include:
Differences in cost of care? Consumers and providers know it’s a problem. 98% of survey respondents across the board agree that healthcare is inconsistent and costs and care vary by location, health system and even within departments at the same hospital.
Two-thirds of consumers don’t believe they would be charged the same for a treatment or condition regardless of where they received care
79% of physicians and nurses acknowledge that cost to the patient influences what treatments they recommend.
87% of all respondents agree there is a lack of transparency in the pricing of healthcare services, including those who are prescribing care or medications
While hospital executives, nurses and physicians are most optimistic that tackling challenges in healthcare variability will lead to better patient outcomes, they are skeptical that it will lead to increased transparency in prices.
Consumers will head to the polls with healthcare in mind. The majority of all four respondent groups say healthcare policy will be a main factor when they cast their presidential votes. Similar majorities say they will vote with their wallet, favoring the candidate who has a plan to respond to rising healthcare costs to them.
The majority of seniors over the age of 65 (87%, in fact) report wanting to age in place as they get older.
Do you have an elderly loved one who’s part of this group? If so, you may have concerns about them staying home, especially if they struggle with health problems.
There are steps you can take to make their home a safe place, though. For example, you can make sure certain senior medical supplies are readily available.
Read on to learn more about the most important supplies the elderly need in their homes. You’ll also learn about the best places to find these supplies.
Essential Senior Medical Supplies
There are a few pieces of equipment that should be present in every senior’s home, especially if they’ve dealt with health issues in the past. The following are some of the most important items to have at the ready:
Personal Alert System
A personal alert system is a must-have for any senior, especially those who are living alone and want to age in place.
With a personal alert system, they’ll be able to contact emergency services right away should they fall or have another accident that requires medical assistance. These systems also provide peace of mind to seniors and their loved ones.
Assistive Equipment
There are many different types of assistive equipment that can be helpful to seniors.
For example, things like toilet risers and grip bars in the bathroom can help protect seniors from falls and provide them with extra stability. Canes, walkers, and wheelchairs provide additional support, as well, and help seniors to remain mobile even as they age.
By Chinmay Singh, co-founder and president, Asparia.
Chinmay Singh
Every medical group today is expected to demonstrate competence and results in population management. Increasingly, pay-for-performance contracts demand that groups utilize data, clinical coordination, and connected technology to improve patient care and patient outcomes. Information in the electronic health records (EHR) is often the glue that binds these initiatives together, enabling the dashboard for what individual patients need and a repository of data that can be analyzed for an entire group.
However, there is a notable gap in EHR capabilities that has been overlooked, up until now. The individual patient’s clinical data should be tapped and used to manage patients when they are not in the doctor’s office – to ensure adherence to manage treatment for chronic illness, for preventive tests and screenings, and for ongoing medical care.
Often called “patient access” functions, these communications today are fragmented, one-way, and for the most part, ineffective. How does the medical group notify the patients who need a particular vaccine? And how do they know that these patients may have actually received the vaccine elsewhere? What happens when preventive tests are due, and the patient doesn’t schedule or maybe doesn’t keep the appointment? What happens when patients are supposed to come back for a follow up in a year, and they don’t?
It’s not for lack of trying that these situations occur. Patient access departments use telephone calls, reminders by mail, e-mail and even texts, with no appreciable increase in consistency in the reduction of no-shows or patient compliance. Patients have good intentions of keeping their appointments, but life intervenes. It’s an inconvenience to them to have to call to re-schedule, and often they just let it go. Staff spending time calling each patient is tedious, time-consuming and expensive – and without a means to keep patients on track, quality of care suffers. Conditions that could have been detected early, may be only found when they are much more serious and expensive to treat. Illnesses that are preventable happen because the test or vaccine wasn’t received. The group’s costs of care go up, and outcomes go down.
Additionally, operational expenses rise. Staff time is wasted in trying to connect with patients by “old school” methods, and each no-show costs the office an average of $200. At a 7-20% no-show rate, a 100-provider health system has revenue leakage of about $10 million a year.
The solution is to adapt new technology like chatbots for example as a way to enable two-way automated communication with patients that taps the data in the EHR, and then communicates with the patient to ensure that the required actions are taken. Intelligent chatbots have modernized the doctor’s office and make convenience equal to that of dealing with the bank or online travel. This is what consumers expect today, and this is what they should be able to experience in health care.
Electronic health record companies such as Epic, NextGen, Athenahealth, AllScripts, Centricity, DrChrono and others have already incorporated these chatbots into their systems. Although awareness of this capability may be low, it is easy and inexpensive to integrate and use. This integration enables “zero friction” implementation and operations; staff do not have to undergo training to learn a new system and can continue to work within the EHR. With no data duplication, the EHR remains the single source of truth for patient data and interactions.
The provider community strives day and night to improve patient outcomes and contribute to the dream of value-based healthcare. However, the complexity of chronic diseases renders strategies ineffective and prevents them from reducing available utilization. In the US, chronic diseases account for 75 percent of all healthcare spending, to the tune of $3.5 trillion. In fact, every 6 out of 10 US adults is living with a chronic condition.
And, the costs are going to inflate in the future as well
By 2030, there will be more than 77 million+ people above 65 that necessitates Medicare coverage, which also calls for better chronic care management measures. If high-risk populations are identified now, the US healthcare can be better prepared to meet care expectations in the future and contain the costs for good. That said, a myopic approach to chronic care isn’t going to cut it. Let’s take a look at the loopholes in current chronic care management programs.
Pitfalls in Chronic Care Management
Fixation on short term goals
Effective chronic care management requires providers to focus on long-term well-being and stabilization needs of patients. However, the Affordable Care Act incentivizes providers for a reduction in 30-day re-admissions post-discharge. To witness a visible and landslide impact in chronic care management, providers must be looking for a mechanism that can track care management for high-risk patients beyond the 30-day readmission policy.
Less accommodation for comorbidities
Multiple chronic conditions have associated comorbidity that can increase the costs in the long run. Healthcare needs to inch to a robust system that takes into account the needs of comorbid patients. Mckinsey research suggests that 71% of patients with heart failure have hypertension, 37% have diabetes, and 53% have hyperlipidemia. These stats indicate that providers have the opportunity to go upstream and engage with these patients while they have a low-morbidity condition.
Inadequate risk stratification
Risk stratification is majorly centered on the needs of high-risk patients and often negates rising-risk patients. While preventive mechanisms for “high-risk” and “rising-risk” patients require a demarcation, specialty care and telehealth don’t promise a similar ROI for both patient pools. Aside from this, additional factors such as Social Determinants of Health are not an integral part of every risk stratification algorithm that results in skewed chronic care management plans.
Fragmented care delivery
A lack of coordination renders chronic care management ineffective and many a time, patients end up receiving clashing treatments that can lead to increased costs.
Primary care vs. specialty care
Primary care providers often face a hard time figuring out when a patient can be successfully managed in a primary care setting or qualifies to be under specialty care. Taking the right call between the two often becomes the reason for higher costs because of an increase in acute care utilization.
Senior living communities depend on human connection and care that serves each resident’s individual needs. But too often, a paper charting system gives way to inefficiencies such as medication mistakes, poor compliance, revenue leaks, and overall headaches for staff and administrators. As a result, senior living communities that rely on paper charts can’t always deliver the level of care they want to provide their residents. This can lead to dissatisfaction among residents.
And if residents are unhappy, community executives are unhappy.
That’s where electronic health records (EHR) come in. They eliminate the pain points of a manual documentation system and make it easier for staff and administrators to focus on the “why” of caring for residents by streamlining the “how.”
Here’s a look at the four main ways EHRs strengthen operational efficiency in senior living communities and enable excellent care for residents.
EHRs Improve Communications and Transparency
Senior living care hinges upon having access to accurate, up-to-date information about a resident’s health. For CNAs to deliver that care to residents, they need to communicate critical information smoothly and in a timely manner.
With a paper documentation system, it’s too easy for important details to get lost in the constant shuffle of folders and paperwork. Poor handwriting can cause confusion. If residents have incomplete clinical profiles, CNAs’ jobs are harder – there’s lots of back-and-forth with other CNAs and digging through file cabinets to find the information they’re looking for.
Compare that with EHRs: CNAs can use EHRs to efficiently record and access information about a resident’s health in real time, on cell phones, tablets, or computers. This information means CNAs can trust the EHR to correctly answer questions about a resident’s medication doses and clinical history.
Plus, long-term record keeping is critical in a senior living community with high staff turnover. EHRs make it easier to onboard new CNAs and help them quickly get acquainted with individual residents’ profiles.
But staff aren’t the only ones who benefit from enhanced communication through EHRs. A centralized and digitized record of contacts invites everyone to the conversation about a resident’s health.
If a resident visits the hospital, medical professionals can forward a hospital intelligence report to anticipate changes to resident services. This elevated communication between senior living communities and hospitals can improve health outcomes – research from the National Institutes of Health shows that EHR use in hospitals decreases readmission rates.
Family members at home want to stay in the loop on their loved ones’ health, too. EHRs can integrate clinical information into senior living family communication portals. That way, family members don’t just hear during visits or after an emergency – they can check in on their loved one’s health as often they please.
In the past, one of the appeals of becoming a doctor was the ability to maintain professional autonomy, with the hopes that this would also offer physicians flexibility and freedom in how they run their medical practices. Unfortunately, today the economic reality is that it will take well over six figures to establish a practice, on top of the average medical school debt accumulated of $150,000 to $200,000, makes creating a profitable traditional private practice a near economic impossibility.
Coworking spaces are not a novelty, and we’ve seen them sprawl nationwide across industries and cities as organizations and technology continue to fundamentally shift how and where we work. Coworking spaces are allowing people flexibility and autonomy and at a significantly reduced cost of running a business. Borrowing from this shared economy model, medical coworking is the disruptive concept needed to revive private practice, making the possibility of self-employment realistic once again by allowing start-up costs to drop from six figures to four, and by offering much needed support to physicians in operations, administration and marketing.
The biggest barrier to entry for a new doctor to start a practice has always been real estate overhead. With a shiny medical degree, but no active patients, doctors are asked to sign multi-year leases, without any promise of immediate or even short term returns on investment. Through my experience as a new physician, it took upwards of two years to establish a solid practice and patient-base, yet during that time I still had student debt and amounting rent and operational costs.
In the coworking model (as offered by Cowork Medical), doctors pay a monthly membership fee allowing them office access, front-desk support, group purchasing discounts and business consulting services. The membership fee gives physicians access to all coworking locations, meaning that a new doctor can have a multi-location practice instantly, giving that doctor the ability to grow a client base quicker and more cost-effectively than ever possible with a traditional model.
For many physicians, business mentorship is critical and the operational support provided by coworking concepts offers immense benefits to physicians entering the business, allowing them to put a stronger focus on their client care rather than dwell on tedious administrative tasks needed to make a business thrive. Doctors are taught to save lives, not how to run a business. Simply giving them an office space to settle in will not address all the vows of establishing and running a practice. Through strategic consulting, members are able to receive immediate access to decades of experience in practice management, learning how to operate and grow a successful practice in addition to strategic marketing tools at a minimal cost.
 Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine[1].
Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine[1].
 The majority of seniors over the age of 65 (
The majority of seniors over the age of 65 (
 Source:
Source: 