By Priya Sabharwal, practice leader, network operations, HGS.
Priya Sabharwal
Imagine a scenario: A patient looking for a new doctor searches her insurer’s online network directory to find a provider her plan will cover. She selects what seems to be the perfect doctor based on her criteria, which could include gender, office location, languages spoken or other qualifications, in addition to being in-network with her health plan.
But there’s a plot twist: The patient eventually learns the doctor she found is not, in fact, the right option for her – but it took her scheduling and arriving at the appointment for her to realize this. It turned out the entry in her insurer’s directory was outdated, and her doctor had moved offices.
This scenario is hardly out of the ordinary. A 2019 Health and Human Services survey uncovered errors in half of the listings in Medicare plans alone. These significant inaccuracies cause issues not just for patients, but for payers and providers, too:
Poor directories are more than just an inconvenience for a member; they also impede their access to necessary care, and can create unexpected medical costs.
A typical health plan is already regularly contacting providers’ offices for many different types of data requests. When they also call to verify provider directory requests, it can create added pain for both sides of the equation. On the payer side, it can create provider abrasion, which could influence whether the provider keeps doing business with that payer. On the provider side, receptionists and office managers are pulled away from their higher-level tasks whenever they stop to answer the phone, leading to short-term frustration and, potentially, burnout.
Payers risk incurring stiff fines and penalties from federal and financial entities, and/or member lawsuits. For example, as of 2016, CMS regulations now permit the agency to fine health plans up to $25,000 per Medicare beneficiary for errors in Medicare Advantage plan directories, and up to $100 per beneficiary for mistakes in plans sold on the Affordable Care Act exchanges.
Poor provider data management hinders effective patient-provider matching, patient satisfaction, and demand conversion through call centers.
If a health plan’s website does not contain thorough, accurate provider information, or reflect correct provider availability, potential patients may go back to the drawing board and select a provider from a different organization.
A lack of complete and reliable provider data about specialists leads to misdirected referrals, and acts as a barrier to patient retention within networks.
So what are some steps payers and health plans can take to create a solid provider data foundation? It starts with fundamentally changing the way we think about, use, enter and maintain data.
Many people call retirement the golden years, and they look forward to it for decades. However, those who make the wrong decisions before and during retirement could find that it’s not as pleasant as they anticipated. Here are some useful tips to help you start your retirement right and increase your happiness and health.
1. Decide When to Start Getting Social Security Benefits
When you retire, you may not want to start withdrawing your Social Security benefits. People who retire early could have to wait to apply for Social Security benefits, and others might not receive the full benefit. According to the Social Security Administration, you can start getting Social Security benefits when you turn 62, but you’ll get about 30% less every month. If you wait and use your retirement savings alone or continue to work for a while, your benefits will increase.
To prevent hospitals from being overwhelmed, states should focus on preventing the spread of COVID-19 at high-risk sites, such as nursing homes, and in high-risk localities, the COVID-19 Policy Alliance—a group of experts brought together by two professors at the MIT Sloan School of Management—said in a presentation released today.
The Alliance also put online a set of data analytic tools to enable states to identify the highest risk facilities and localities—those with clusters of individuals over 65 or with relevant health issues.
The Alliance analysis indicates that one of the factors possibly leading to the high fatality rate in Italy was that sick people from areas with concentrations of high-risk individuals overwhelmed hospitals, creating a domino effect that led to skyrocketing death rates. The Alliance has developed tools to identify institutions and counties in every state in the U.S. that have the same characteristics as the points in Italy that put its health care system into a tailspin.
For example, the data tools not only show where nursing homes are and how many people reside in them, but show which nursing homes have had the most problems previously with infections. For counties, the tools show not only areas with high numbers of elderly, but also those with high numbers of individuals of all ages suffering from diabetes, obesity and other conditions that create COVID-19 risk.
A 15-minute webinar describing the Alliance’s tools and recommendations for U.S. federal, state and local policymakers is here. The webinar expands on a slide deck that lays out the analysis and guidance.
The COVID-19 Policy Alliance was launched on March 11 by Professors Simon Johnson, the Ronald A. Kurtz Professor of Entrepreneurship, and Retsef Levi, the J. Spencer Standish Professor of Operations Management. They pulled together a team of experts from across MIT and elsewhere to analyze the available data on the pandemic. The tools will be updated as more data and analysis are available.
Levi said, “We want to help states make data-based decisions that can save lives. Focusing on the sites and areas that are most likely to lead hospitals to crash is key.”
Johnson said, “Hospitals are a critical line of defense in the ongoing battle against COVID-19. We must focus now on preventing our world-renowned hospital systems from collapsing.”
By Chrissa McFarlane, CEO, Patientory, and Jonathan Fuchs, FACHE, member of the board, Patientory Association.
As we approach a new decade, there are a plethora of predictions being made around the future of the healthcare industry. Healthcare’s journey to value will, of course, continue, however, industry challenges and boundaries (i.e. competitive pressure, lack of transparency, limited patient access and erosion of trust) are still areas of concern and opportunity as the industry progresses.
My education, experience, and journey as an entrepreneur led me to create Patientory to empower consumers with an application they can use to improve their overall health and well-being. We are the world’s first healthcare cryptocurrency and HIPAA-compliant blockchain network, with more than 50 nodes registered worldwide.
I recently sat down with Jonathan Fuchs, FACHE, veteran healthcare executive, who also serves as a board member for the Patientory Association. With more than four decades of experience in healthcare management and operations, Jonathan’s expertise in health information technology, data analytics has allowed him to focus on assisting healthcare startup companies on reimbursement strategies, the impact of data and analytics on value-based care.
Chrissa McFarlane
Chrissa McFarlane: Jonathan, thank you so much for sitting down with me to talk about Healthcare 2030. Taking a look back at how the healthcare industry has advanced over the past two decades is astounding. However, as we look ten years ahead, I believe a consumer-centric healthcare system will be crucial for industry growth. What do you say to this and how do you believe technologies such as blockchain will lead the way in advancing this mission?
Jonathan Fuchs: Chrissa, of course. To your question, health information exchange will be critical in advancing the healthcare industry and honing in on the consumer-centric approach over the next decade. Blockchain will essentially help with interoperability by streamlining efficiencies, making health care an achievable and cost-efficient reality for all. The ability to transmit patient records safely and securely will, in turn, allow patient data to be viewed by hospitals and other providers in any participating region, city or country meaning the potential of blockchain will be boundary and boundless. In addition to this, the issues of cybersecurity are also top of mind. The ability to encrypt data (specifically on a healthcare blockchain) prevents unauthorized parties from accessing and reading patient data, even if they are able to access the blockchain itself.
Blockchain technology will help create better privacy standards within the industry.
Chrissa: What would you say are some of the roadblocks to Blockchain adoption?
Johnathan: Until the ability for various healthcare information technology systems to exchange, interpret and use data cohesively occur, we will continue to see latency in the adoption of Blockchain. The very structure of the technology enables data exchange to happen at a higher level of transfer. Which, currently, electronic servers and EHR systems are not set up to handle the volume or power requirements. Another roadblock is scalability, blockchain is expensive (for now)and at this point requires more power resources to handle the speed at which it operates. That’s not to say this will always be the case, but it’s definitely true today.
Chrissa: Historically, healthcare has been slow to change. Many would argue that healthcare should be more realistic than futuristic. What do you say to this?
Throughout this challenging time of the COVID-19 pandemic, Glooko, a diabetes software company that enables people with diabetes and clinicians to manage care in real-time, is committed to helping ensure the health and well-being of people with diabetes, their caregivers, and their healthcare professionals. Glooko is therefore taking action to serve the global diabetes community by providing a no-charge remote-care solution that provides live patient-to-clinician connectivity.
As many efforts undertaken in our communities are aimed at reducing the chances of being exposed to and spreading COVID-19, individuals who have chronic conditions like diabetes and contract the virus appear to be at a higher risk for developing complications; as such limiting exposure is critical.
For certain appointments, healthcare professionals may determine that the patient and their care team would be best served by a remote review of the patient’s personal diabetes data and a corresponding telehealth consult, reserving in-office visits only for those appointments where a patient’s medical status truly requires in-person treatment.
To minimize the risk to people with diabetes during this time by broadening access to remote medical appointments with healthcare providers, Glooko is offering its secure, privacy-protected remote-care solution at no charge to medical clinics and people with diabetes as a public service until the greatest threat of the pandemic has subsided.
This public service is being made available to medical clinics and people with diabetes in countries where Glooko technology is already provided. Interested medical clinics and people with diabetes can learn more about how to access the Glooko remote-care solution at www.glooko.com.
GeneratorWorks, a technology company with a suite of healthcare software and hardware products, has announced a partnership with clinical algorithm platform SmartDocMD. Together, they have released SecurePass, a digital COVID-19 risk stratification and screening survey.
With bold and proactive steps, SecurePass creates a solution that effectively surveys patients and healthcare communities to identify possible COVID-19 risks. With this information at hand, healthcare facilities can better inform and remotely support those showing possible high-risk indicators.
SecurePass is powered by SmartDocMD’s clinical algorithms that combine CDC Guidelines for risk assessment, patient symptoms, and medical comorbidities to identify and help segregate higher-risk patients.
The product plugs in patient demographics, geolocation, risk factors, illness symptoms, severity and comorbid conditions that can be viewed in real-time and shared with GeneratorWorks portfolio of products as well as infectious disease teams, including the Center for Disease Control.
SecurePass has the strength of the GeneratorWorks suite of healthcare software and hardware products and is even stronger when tied to:
GetOnHealth, a virtual clinic platform where patients can be assessed and connected via a virtual visit to their primary care or other necessary doctors.
Queue, currently in service to over 50 hospitals nationwide, helps healthcare providers give their patients an overarching positive experience as an organized intake, check-in, and transfer system.
“Our world has changed with the current COVID-19 pandemic, and health systems are becoming overwhelmed” states CEO Blake Squires. “Quick-to-act and scalable digital tools need to be implemented. Understanding community health and provider needs are critical to ensuring the safety and ongoing operations of healthcare facilities and workers. With our collaboration to create SecurePass, we can do just that, while keeping patients informed, connected and safe.”
“As health systems are scrambling to contain COVID-19, bold, collaborative action is our only course,” explains Brian D’Anza, MD, President and Founder of SmartDocMD. “SmartDocMD’s clinical algorithms work within SecurePass to make sure the right patients are being seen at the right time. It ensures health systems can triage patients before they spend hours sitting in the ER, clinic, or another hospital site, which reduces transmission of this highly contagious disease.”
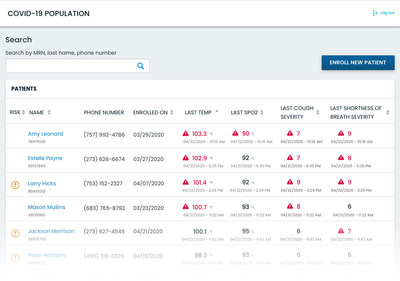
As part of Validic‘s efforts to address the global coronavirus (COVID-19) outbreak, the company launched a real-time monitoring solution designed to observe, analyze and triage individuals remotely for the emergence of COVID-19 symptoms.
COVID-19 Home Monitoring tracks a person’s body temperature, difficulty breathing, cough frequency and oxygen saturation. The solution provides real-time analysis and escalation of critical health data to care management teams, public health officials and/or human resource administrators.
Dashboard panel view to triage patients and view individuals’ real-time and trending home health data. The dashboard allows clinicians or administrators to enroll new individuals; set alerts and triggers; identify trends quickly; and, search individuals based on status and latest readings.
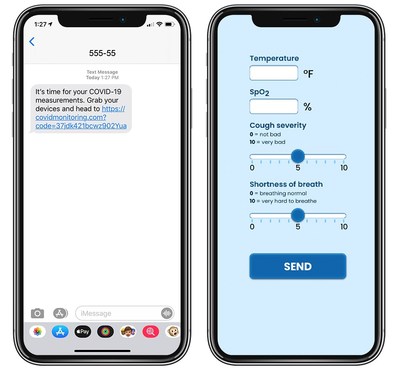
Patients submit health data via secure text or email message. Individuals share daily –& or more regular – updates on symptoms: body temperature, difficulty breathing, cough frequency, and oxygen saturation.
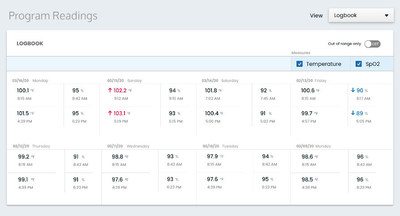
Patient logbook view of current and historical biometric readings and symptoms.
In an effort to empower people on the frontlines of this health crisis, the solution is designed for rapid deployment and scale:
Triage individuals, monitor health metrics and codify next steps
Bulk enroll thousands of individuals quickly
Automate measurement reminders via text and/or email
Triggered alerts will notify program administrators or clinicians as a person’s symptoms worsen, improve, or remain static – or as a quarantine period ends with no symptoms present.
“Given our expertise in personal health data and remote patient monitoring, we’ve been working to quickly develop and launch a custom COVID-19 solution that allows for proactive, remote interventions using real-time data. At no time in recent history has there been a higher imperative to use distance monitoring to keep people alive and healthy,” Drew Schiller, CEO of Validic, said.
“Everyone’s safety, especially those individuals who cannot self-isolate – like our emergency responders, nurses, and sanitation workers – need to be a foremost priority, especially at this time. We want all healthcare professionals and employers to be able to leverage industry-leading remote monitoring capabilities to help people impacted by or potentially exposed to coronavirus.”
As health systems, health plans and employers across the country continue to face an urgent need to monitor people for the emerging symptoms of COVID-19, Validic is offering this solution with a flexible, month-to-month plan that ensures organizations can access the platform without financial constraints.
Companies in the healthcare field have a lot of unique challenges compared to those in other industries. For example, while healthcare companies still, of course, have the same universal business challenge of attaining – and maintaining – profitability, they also have specific healthcare-related challenges such as:
maintaining positive patient outcomes
following safety and privacy regulations
keeping up with advancements in healthcare technology
retaining and attracting talent despite a major healthcare talent crisis: too many experienced workers are retiring / leaving healthcare and there’s not enough incoming talent to fill the void. As a result, the healthcare industry will add about 2.3 million new jobs from 2016 to 2026, which is three times more than other industries (S. Bureau of Labor Statistics)
While each of the above challenges is important, the healthcare talent crisis has the potential to wreak the most damage to healthcare companies, since every organization needs talent to do…well, anything. And more specifically, it’s not uncommon to find leaders in the healthcare industry feeling stuck when it comes to recruiting talent and leveraging employer branding to help them do so.
Here’s how to approach employer branding in healthcare:
Consolidate brand mindshare in your current employees
Sometimes it costs more to recruit, hire and train new employees than it does to maintain your existing work force. This is one reason why you will want to place a priority on consolidating mindshare amongst current workers so that when you do need to recruit new employees, you’ll be able to take on that task more easily and in a more focused way. In other words: if you get your current employees unified and supportive of your company’s employer brand from the inside out, showcasing your company to potential candidates gets to be MUCH simpler.
Do this by displaying your company’s branding within the organization’s walls (on signage as well as printed materials from stationary to logos on coffee mugs) as well as in all electronic documents to clearly establish and reinforce your identity among existing talent. Also, you should find ways to communicate and celebrate your organization’s purpose — your reason for existing! — by sharing your mission statement and code of values any chance you get.
Monitor and manage your reputation as an employer
Your healthcare employer brand ought to help you attract better candidates who want to be associated with a top company. So, employer branding includes flaunting all of the benefits you offer to your employees, staying on top of any press and news that your company gets so that there’s no PR damage, and actively responding to your online company reviews from current and former employees to show that you’re a thoughtful employer with a good reputation. You can count on attracting much more interest from top-quality candidates when your employer brand reputation is nothing short of stellar.


 To prevent hospitals from being overwhelmed, states should focus on preventing the spread of COVID-19 at high-risk sites, such as nursing homes, and in high-risk localities, the COVID-19 Policy Alliance—a group of experts brought together by two professors at the MIT Sloan School of Management—said in a presentation released today.
To prevent hospitals from being overwhelmed, states should focus on preventing the spread of COVID-19 at high-risk sites, such as nursing homes, and in high-risk localities, the COVID-19 Policy Alliance—a group of experts brought together by two professors at the MIT Sloan School of Management—said in a presentation released today.



 By Dr. Sarah Müller, managing director,
By Dr. Sarah Müller, managing director,