The cost of healthcare disparities has been long and deeply felt by patients and their families, but it wasn’t until the high rates of COVID-19-related hospitalizations and deaths among persons of color made headline news that the broader societal impacts of health disparities became more widely known. In response, health systems are prioritizing health equity and leveraging new tools and data to support their work.
At a physiological level, the presence of underlying chronic disease increases the risk presented by COVID-19. The incidence of chronic disease(s) is increasing among all Americans, but the prevalence is much higher among the poor, which includes a higher percentage of individuals of color compared to the overall White population.[1] Health inequities among communities of color are further exacerbated by structural and institutional racism, which experts say “harms health” because of negative factors in their physical, social, and economic environments and a propensity to develop maladaptive coping behaviors (e.g., smoking, alcohol, etc.)[2].
A Community-Level Issue
Increasing rates of chronic disease create a self-reinforcing cycle that threatens the well-being of entire communities (and the health systems that serve them). Individuals suffering from chronic disease have higher rates of absenteeism,[3] which limits their wealth building potential, the productivity of their employers and the tax base of their communities. This, in turn, increases poverty and the impact of the social determinants of health (SDOH) that contribute to higher rates of chronic disease. The combination of chronic disease (as an inflammatory condition) and the psychological stress of racism have been shown to cause physiological changes that raise the risk of contracting additional chronic diseases.[4]
Hospital performance is also tied to economic well-being. Research documents a correlation between the quantity and quality of local economic resources and the clinical performance of hospitals, which under value-based payment models, can also impact financial performance.[5] With chronic disease responsible for nearly 90% of national health expenditures,[6] it’s continued rise threatens our national economy and the ability to fund needed healthcare for the poor and aging. In other words, this is not just a social issue; it is an economic imperative. A 2021 Institute for Healthcare Improvement (IHI) study found that 58% of healthcare executives ranked health equity as one of their organization’s top three priorities, up from 25% in 2019.
Health equity is a focus of providers, regulatory agencies, and payers as they seek ways to eliminate care disparities across race and ethnicity, gender, sexual orientation, and socioeconomic status lines. Its significance is further impacted by new quality-based care models beyond those established by the Patient Protection and Affordable Care Act of 2010.
The challenge for many healthcare organizations participating in these new reimbursement models is how to view health equity and social determinants of health (SDoH) to understand the actual value of this information. Often overlooked is that healthcare organizations’ coding and revenue cycle management (RCM) departments already aggregate information that can help better understand inequities in care delivery and health equity across their patient populations.
A Primer on SDOH Impacts
SDoH impact many health risks and outcomes, which is why this data is vital for clinical care and reimbursements. Defining factors can include anything from geography, race, gender, and age to disability, health plan, or any other shared characteristic. Of increased importance, SDoH issues are most often experienced by the most vulnerable members of society: the poor, less educated, and other disadvantaged groups.
SDoH is linked negatively with outcomes, including higher hospital readmissions, length of stay (LOS), and increased need for post-acute care. Value-based payment programs, therefore, may penalize organizations that disproportionately serve disadvantaged populations if they do not collect and respond to SDoH data.
For example, addressing food insecurity — a key SDoH data point — by connecting patients to programs like Meals on Wheels, Supplemental Nutrition Assistance Programs (SNAP), or food pantries is proven to reduce malnutrition rates and improve short and long-term health outcomes.
In the case of SNAP, which is the primary source of nutrition assistance for more than 42 million low-income Americans, participants are more likely to report excellent or very good health than low-income non-participants. Low-income adults participating in SNAP incur about 25% less medical care costs (~$1,400) per year than low-income non-participants.
The COVID-19 pandemic exposed the true costs, human and otherwise, of health disparities, as low income and minority populations suffered disproportionately from the virus. Blacks, Native Americans and Hispanics were 2% to 3.3% more likely to be hospitalized or die from the virus compared to non-Hispanic Whites, primarily because of a higher prevalence of underlying disease states (hypertension, obesity and Type II diabetes) caused by relative lack of access to the so-called social determinants of health: good paying jobs, healthy food, safe housing, and transportation, among others.
As with so many aspects of the pandemic, supply chain is front and center in the fight, which is playing out on their home turf, literally. Once again, supply chain is also getting noticed in the executive suite, as the boards of trustees for America’s hospitals prioritize health equity in preparation for taking on more risk for the populations they serve under value-based reimbursement programs. Here are few ways they are making a difference.
1. Bringing Diversity Home
Supply chain professionals have long sought to increase their spend with diverse suppliers, defined primarily as those that are women, minority, veteran, or LBGTQ-owned. That data is tracked and often used to support grant applications. More recently, transparency around that spend is being mandated. In California, for example, Assembly Bill 962 (AB 962) requires all hospitals meeting a certain threshold to report how much they spend with diverse suppliers each year.
But for many health systems, diversity is not enough. They want to make sure they are using their purchasing power to support the health and well-being of local communities where the patients they serve live. Spending in local communities has a multiplier effect. For example, investing in a local business supports job creation; in turn the wages for those employees generate local tax dollars and increase their ability to spend and generate wealth in their own communities.
The healthcare business of LexisNexis Risk Solutions announced a collaboration with Carrot Health, a provider of solutions powered by consumer and healthcare data. The collaboration enables Carrot Health to incorporate social determinants of health (SDoH) data from LexisNexis Risk Solutions into its SDoH data and analytics software platform to guide payer and provider decisions around member engagement and health management.
Through this collaboration, Carrot Health will integrate clinically-validated SDoH attributes from LexisNexis Risk Solutions into its existing Social Risk Grouper (SRG) taxonomy and other predictive models that leverage vast consumer and healthcare data. These insights will inform consumer-centric strategies to improve health outcomes, reduce costs and prevent readmissions.
Kurt Waltenbaugh
“Consumer attributes are among the most powerful factors influencing health outcomes, creating barriers and inequities that prevent populations from leading their healthiest lives. Carrot Health’s SRG harnesses this information to measure and monitor social determinants of health at the individual level, providing comprehensive insights our customers need to design strategies for identifying and closing gaps in care while providing a more personalized member experience,” said Kurt Waltenbaugh, CEO, Carrot Health. “We chose LexisNexis Risk Solutions after extensive evaluation and testing because their consumer data proved to be the most accurate and comprehensive in the market. We are excited about this addition to our platform as we continue to help payers improve member health.”
Carrot Health’s platform harnesses clinical, social, economic, behavioral, and environmental data to deliver insights for growth, health, and quality, providing health plans with a 360-degree view of their members. Carrot Health is delivering the healthcare industry’s first solution for consumer insights at scale, along with individual-level SDOH scoring and monitoring for every adult in the United States.
This scoring model helps predict the likelihood of an individual having an adverse health outcome due to their SDoH profile. The data from LexisNexis Risk solutions will augment Carrot Health predictive models, that already includes consumer data, ICD-10 Z-codes, publicly available health indicators, claims, survey responses, and other proprietary data ? providing unmatched accuracy to a scoring model.
By Julie A. Pursley, MSHI, RHIA, CHDA, FAHIMA, director of health information thought leadership, AHIMA.
Julie A. Pursley
Reading news articles about vulnerable communities disproportionately affected by COVID-19 has been heartbreaking. My organization, the American Health Information Management Association (AHIMA), believes that social determinants of health (SDOH)—the socio-economic behavioral elements that affect health—play in role in explaining why poorer communities have experienced more negative impacts during the pandemic than other areas. We also believe it’s vital for SDOH information to be recorded in medical records.
It’s not difficult to imagine why low-income Americans may face increased exposure to the novel coronavirus. Perhaps most critically, people experiencing poverty are more likely to not have health insurance or be underinsured.
In addition, while many office workers have worked from home during the pandemic, people who earn lower incomes often work in public-facing jobs like restaurants and grocery stores and have no choice other than to take public transit to get to work. And the millions of Americans who have lost jobs may be dealing with food insecurity and a lack of money available to secure food and other goods at home.
Communities of color often comprise low income workers who encounter many of the situations mentioned above (and more). At AHIMA we support collecting race and ethnicity data for optimal public health reporting because recording SDOH information in a patient’s medical record can lead to better healthcare outcomes. SDOH information in a patient record offers providers a more complete story and can influence how they approach treatment, education, and care management.
“We’ve had physicians across our practices reach out to patients living alone during this time of social isolation, those who were identified as potentially being isolated and without support,” William Torkildsen, MD, chairman at South-Texas-based independent physician association Valley Organized Physicians (VOP), recently told the Journal of AHIMA. “We recorded those results and have been able to take action on the patient’s behalf, connecting them to necessary resources.”
By April Gill, senior vice president, solution management, Welltok.
The future of COVID-19 remains a giant question mark right now. But what is clear in this uncertain time is the significant impact everyday factors, commonly called social determinants of health (SDOH), have on a person’s health. Literature shows that up to 70% of a person’s overall health is driven by SDOH, including factors like race, income, education level and more. Knowing about these factors can improve how providers keep patients healthy year-round, but also how they engage, counsel and treat patients as individuals during a crisis like the one we are currently experiencing.
If providers understand what kinds of SDOH their patients are facing, they can better understand what health risks they have today, as well as to anticipate their future needs and risks. They can use this insight to tailor what information they share with whom, using the most effective communications channels.
Consider an elderly patient who does not own a car and relies on public transportation for everyday needs. Before COVID, a provider may have leveraged this insight to connect them to Lyft to get to a clinical appointment.
Now, a provider with this insight would likely do much more – have a telehealth appointment instead, connect them with local volunteers who will deliver groceries so they can maintain a healthy diet without leaving home, and email them facts about how to minimize risk while using public transportation to pick up a prescription, if absolutely necessary. This is just one example of how providers can improve patient care and support by understanding what they experience every day.
But are patients aware of the impact SDOH have on their own health? To find out, Welltok conducted a survey of over 2,000 consumers earlier this year, to get their views on what factors they think affect health, and which ones they would share with their provider. Surprisingly, consumers underestimated how much SDOH influenced their overall health and wellbeing – responding that they only make up about 50% of a person’s overall health. (It’s really 70%). They did have a good understanding of some factors that drive health status – like type of work or who they live with – but not more than half did not understand how daily factors like length of commute also play a role.
Not surprisingly, three out of four people also told us they experienced a change in life in the last year that impacts health. The top ones were a change in 1) stress level, 2) annual income and 3) the amount of debt they have. With most provider interactions being episodic in nature, the opportunity to get to know patients at a personal level and/or stay apprised these changes is extremely difficult. Building off this, consumers were asked to list who they would share these life changes with.
It is encouraging to see many healthcare systems and payors focusing on the impact of social determinants of health (SDoH) and looking for ways to partner with community-based organizations to address and improve these issues locally. Although this is a necessary step, I believe that providing access or referrals to community organizations is not the full answer.
While healthcare systems can provide referrals and connect patients to resources such as food banks or employment resources, it may not be enough to create individual engagement and empowerment to use those resources. We more fully need to appreciate the role played by the environment in which we grow up and the choices available to us in shaping how we respond toSDoH factors as individuals.
As part of an innovation center where we align data science withSDoH to help systematically disadvantaged individuals, I’ve been witness to projects and research that point to the theory of individual resiliency as part of the equation. The American Psychological Association defines individual-level resilience as the process of adapting well in the face of adversity, trauma, tragedy or threats.[1]
A review of the research on resilience by the WHO found that an individual’s ability to successfully cope in the face of significant adversity develops and changes over time, and that interventions to strengthen resilience are more effective when supported by environments that promote and protect population health and well-being. Further, supportive environments are essential for people to increase control over the determinants of their health.[2]
Also, in addition to traditional resilience methods, the emergence of methods to assess an individual’s capacity for self-care are adding significant insights into personal determinants of health. In particular, the needs of the growing population of complex patients with multiple chronic conditions calls for a different approach to care.
Clinical teams need to acknowledge, respect and support the work that patients do and the capacity they mobilize to enact this work, and to adapt and self-manage. Further, clinical teams need to ensure that social and community workers and public health policy advocates are part of the proposed solution. Researchers at the Mayo Knowledge and Evaluation Research (KER) Unit and the Minimally Disruptive Medicine (MDM) program led by Dr. Kasey Boehmer are developing qualitative methods and measures of capacity and individual’s ability for self-care.
Take post-traumatic stress disorder (PTSD), as an example. It has been estimated that around 50-60 percent of people in the US will experience severe trauma at some time in their lives. Around one in 10 goes on to develop PTSD, which is permanent in a third of cases.
But some people who have lived through major traumatic events display an astonishing capacity to recover.[3] A complex set of factors can be attributed increasing an individual’s resiliency to trauma including their personality, their individual biology, childhood experiences and parental responses, their economic and social environment as shaped by public policy, and support from family and friends.
Addressing the social determinants of health (SDoH) in communities is a hot topic of conversation in healthcare. The industry has bought into the theory that 20 percent of an individual’s health is determined by clinical care and the rest by social, economic, genetic and behavioral factors. But perhaps more importantly health systems need to recognize that they can’t solve this issue on their own.
From my perspective at PCCI, I’ve seen an increase in value-based contracting models in recent years, and health systems and physicians are looking beyond the four walls of their institutions to build relationships with outpatient, behavioral health, post-acute care, and now non-medical providers. The number and types of collaboratives between health systems and non-traditional providers has been growing over the past several years with a recent report gathering information on more than 200 different partnerships between hospital and community-based organizations across the country.
But while health systems may be embracing community provider relationships, I believe that sustainable success in addressing social determinants of health requires a fundamental shift in the way health systems view their role in improving the health of their communities.
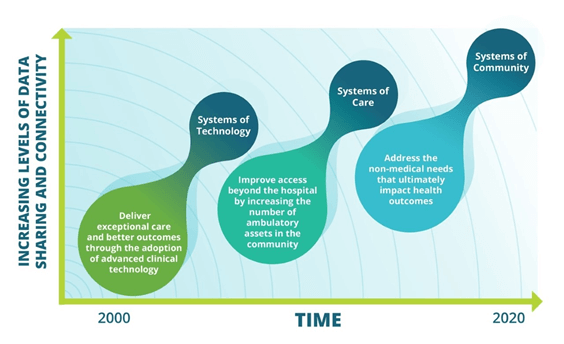
Over the past ten to fifteen years there has been an evolution in how health systems have approached improving health outcomes. Initially health systems focused on providing high-tech solutions for care delivery such as robotic surgery, and advanced imaging techniques. Then to meet the need for increased access and demand for outpatient services, health systems seeded service areas with ambulatory surgery centers, urgent care, retail clinics, and physician offices.
In each of these evolutions the strategies centered on a solution created by the health system alone. And one could argue that the main beneficiaries of these investments were often the health systems themselves – increased market share, improved reimbursements. But such a self-centered approach will not work when addressing social determinants where the root causes lie outside the four walls of the health system.
Effectively creating a system of community will require a collaborative mentality from health systems. While they may have power and influence to gather partners to the table, execution of successful interventions lies with social services and community-based organizations that are the experts in understanding and helping individuals address social needs. Even if not leading, health systems should still be active participants in this work. Indeed, there are areas where their contributions to the organization of partners is critical:





 The future of COVID-19 remains a giant question mark right now. But what is clear in this uncertain time is the significant impact everyday factors, commonly called social determinants of health (SDOH), have on a person’s health. Literature shows that up to 70% of a person’s overall health is driven by SDOH, including factors like race, income, education level and more. Knowing about these factors can improve how providers keep patients healthy year-round, but also how they engage, counsel and treat patients as individuals during a crisis like the one we are currently experiencing.
The future of COVID-19 remains a giant question mark right now. But what is clear in this uncertain time is the significant impact everyday factors, commonly called social determinants of health (SDOH), have on a person’s health. Literature shows that up to 70% of a person’s overall health is driven by SDOH, including factors like race, income, education level and more. Knowing about these factors can improve how providers keep patients healthy year-round, but also how they engage, counsel and treat patients as individuals during a crisis like the one we are currently experiencing.