Healthcare organizations operate in an increasingly complex financial environment where accuracy, speed and compliance directly impact profitability. As reimbursement models evolve and administrative burdens increase, hospitals and provider groups are turning to automation and artificial intelligence to optimize financial performance across the entire revenue cycle.
What Is Revenue Cycle Management?
Revenue cycle management is the end-to-end financial process healthcare providers use to track patient care, from initial appointment scheduling and registration to final payment collection. It includes multiple interconnected stages such as coding, billing, claims submission, payment posting and denial management.
Each stage is vulnerable to inefficiencies and manual errors that can disrupt cash flow, where even small inaccuracies in coding or eligibility verification can lead to claim rejections or payment delays. As such, challenges in this cycle can have a significant financial impact on healthcare organizations.
For example, according to the Centers for Medicare & Medicaid Services (CMS), the Medicare Fee-for-Service program alone recorded $28.83 billion in improper payments in fiscal year 2025, with an improper payment rate of 6.55%. These errors include documentation gaps, coding inaccuracies and billing mistakes, issues that originate directly within the early stages of the revenue cycle.
How Automation Impacts Revenue Cycle Management
Modern revenue cycle management automation is reshaping how healthcare organizations manage financial operations by embedding AI and machine learning into core workflows.
1. Streamlining Patient Registration and Eligibility Verification
The revenue cycle begins at registration, where inaccurate patient data can trigger downstream billing issues. As such, automation tools now validate insurance eligibility in real time, reducing manual verification work. AI-driven systems can also flag missing or inconsistent demographic information before claims are created, significantly reducing avoidable denials.
Denials are one of the most costly challenges in healthcare finance, so automation transforms denial management from a reactive to a proactive process. Machine learning models analyze historical denial patterns to identify root causes such as coding errors, eligibility issues or payer-specific rules.
These insights allow organizations to prevent future denials rather than simply correcting them after the fact. Denial management and prevention provide measurable improvements in turnaround times, patient financial clearance and self-service collections.
This proactive approach reflects a core theme from the 2026 AGS Health Summit, which identified front-end denial prevention, powered by a “hybrid intelligence model” of AI supporting skilled staff, as a primary driver of financial returns.
2. Enhancing Medical Coding Accuracy and Efficiency
Medical coding is a critical but complex and error-prone part of the revenue cycle management process. It involves translating clinical documentation into standardized codes used for billing and reimbursement, so even small gaps or interpretation errors can lead to claim denials, delays or compliance risks.
As such, automation is increasingly used to support this process, helping identify relevant clinical details within patient records and automate encoding. These tools help reduce manual workload while also improving speed, consistency and accuracy. A successful automation can save hours and possibly days of work. For example, a 45-second file transfer in an old method can take no more than a second with new workload automation software.
Additionally, AI algorithms trained on large billing datasets can identify discrepancies in submitted claims to detect potential fraud and recommend corrective actions, which enhances transparency and compliance.
3. Improving Billing and Claims Submission
Billing errors and incomplete claim submissions are major contributors to delayed reimbursement. As such, automation platforms streamline claims generation by validating payer rules before submission. This includes checking for missing modifiers, incorrect patient data and payer-specific formatting requirements.
In fact, there can be an increase in reimbursement accuracy by up to 25% with AI. By reducing the number of claim failures, healthcare organizations improve first-pass acceptance rates and shorten revenue cycles.
4. Supporting Decision-Making With AI
Beyond task automation, AI adds a layer of predictive intelligence to revenue cycle management operations. Analytics can forecast reimbursement timelines, estimate denial risks and identify revenue leakage points across departments. This allows finance and organizational leaders to make data-driven decisions that improve both operational efficiency and financial outcomes.
The Future of Revenue Cycle Management
Automation is fundamentally reshaping healthcare financial operations by streamlining workflows across the entire revenue cycle. From registration to denial management, intelligent systems reduce friction, improve accuracy and accelerate reimbursement.
As healthcare continues to shift toward value-based care and increased financial accountability, adopting advanced technologies in revenue cycle management will be essential for long-term sustainability and profitability
By Leigh Poland, RHIA, CCS, CDIP, CIC, is Vice President – Coding Services, Clinical Quality, and Education, AGS Health
The latest ICD-10 update may look insignificant to many healthcare organizations. There are no sweeping diagnosis code additions, no major guideline rewrites, and no dramatic restructuring of the classification system at first glance.
That perception could become a costly mistake.
The April 2026 ICD-10 changes introduced by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) are deceptively quiet. While the diagnosis code set itself remains largely untouched, the update alters something far more consequential: the decision-making framework coders use to determine sequencing, coexistence, and classification relationships. In practical terms, the update shifts more responsibility onto coder judgment, documentation precision, and organizational oversight.
For health systems already navigating staffing shortages, denials pressure, increasing payer scrutiny, and growing dependence on encoder technology, even modest classification logic changes can create operational instability.
The Real Change Is Not the Codes
The 2026 ICD-10-CM release includes no additions, deletions, or revisions to diagnosis codes. The Official Coding Guidelines also remain unchanged. But focusing only on code counts overlooks where the actual disruption is occurring.
The most meaningful changes involve instructional notes, exclusions, and indexing logic embedded within the classification system itself. These structural revisions alter how diagnoses relate to one another and how coders determine sequencing priorities.
Historically, ICD-10 relied heavily on embedded hierarchy through directives such as “code first” and “use additional code.” Those instructions created relatively rigid sequencing expectations. The April update softens several of those relationships by replacing them with “code also.”
That wording change appears minor. Operationally, it is not.
“Code also” removes automatic sequencing hierarchy and places greater emphasis on the clinical circumstances of the encounter. As a result, two experienced coders reviewing similar documentation may now reasonably arrive at different sequencing conclusions.
That variability introduces downstream risk for MS-DRG assignment, reimbursement consistency, quality reporting, and audit exposure.
Hypertensive Emergency Becomes a Judgment Call
One of the clearest examples appears in category I16.1 for hypertensive emergency.
Previous instructional language reinforced sequencing expectations around the hypertensive crisis itself. Under the revised structure, coders must now determine whether the hypertensive emergency or the associated complication represents the principal reason for admission.
In real-world inpatient settings, that distinction can materially alter reimbursement outcomes.
If the case emphasis shifts toward complications such as acute kidney injury, myocardial infarction, encephalopathy, heart failure, or cerebral infarction, the resulting DRG assignment may change significantly.
What was previously more standardized now becomes more interpretive.
For revenue integrity teams, this creates a new challenge: ensuring consistent organizational logic across coding staff, CDI specialists, and auditing functions.
Expanded Coding Combinations Increase Complexity
Another major change involves the conversion of multiple Excludes1 notes to Excludes2 notes. Within ICD-10 methodology, this distinction matters enormously.
Excludes1 notes prohibit reporting two conditions together because they are considered mutually exclusive. Excludes2 notes acknowledge that conditions may coexist when clinically appropriate.
The April revisions expand the number of valid diagnosis combinations across several clinical areas, including hematologic disorders, respiratory failure, and substance-related conditions.
That expansion creates both opportunity and risk.
On one hand, organizations may now capture clinical complexity more accurately. On the other, newly permissible combinations may attract increased payer attention if documentation does not clearly establish coexistence and medical necessity.
Respiratory failure coding illustrates the issue well.
The revision affecting postprocedural respiratory failure now allows certain respiratory failure conditions to be reported concurrently when documentation supports both diagnoses. Depending on sequencing and present-on-admission indicators, these changes can influence CC/MCC assignment and case severity calculations.
Increased flexibility sounds beneficial until organizations realize it also increases variation.
Technology Alone Will Not Solve This
Many organizations assume encoder systems will absorb these changes automatically. That assumption deserves caution. Encoder logic can support compliance, but it cannot fully resolve interpretive ambiguity introduced by structural classification changes. When sequencing hierarchy is loosened, technology becomes more dependent on human documentation quality and coder judgment.
This is particularly important as hospitals continue expanding the use of AI-assisted coding workflows.
Automation performs best in environments with stable and predictable rules. The more classification systems rely on nuance, contextual interpretation, and clinical prioritization, the more critical human oversight becomes.
The April ICD-10 update quietly reinforces that reality.
Healthcare organizations increasingly pursuing autonomous coding strategies may find that classification logic changes expose gaps in governance, validation, and audit readiness.
While the diagnosis side of the update focuses on logic restructuring, ICD-10-PCS continues expanding to capture emerging procedural complexity. New codes support advancements in cardiac pacing technologies, including conduction system pacing techniques involving ventricular septal lead placement.
Additional updates improve specificity for hepatobiliary and pancreatic drainage procedures by distinguishing transpapillary and transmural approaches commonly used in advanced endoscopy.
The update also expands reporting capabilities for reconstructive urologic procedures, rehabilitation therapies, electrotherapeutic modalities, and new technology interventions involving biologics, vascular scaffolds, gene therapies, and immunotherapies.
These additions reflect a continuing challenge for healthcare organizations: clinical innovation is moving faster than many operational infrastructures can adapt.
The significance of this update extends beyond HIM and coding operations. Sequencing variability influences reimbursement predictability. Documentation inconsistency affects denial vulnerability. Coding interpretation impacts publicly reported quality measures and risk adjustment performance.
In other words, structural coding logic changes eventually become enterprise financial and operational issues.
Organizations that dismiss this release because it lacks major code volume changes may underestimate its cumulative effect over time.
The healthcare industry often focuses attention on large regulatory overhauls while overlooking smaller classification refinements that quietly reshape operational behavior. This update falls squarely into that category.
The Organizations Most Likely to Struggle
The greatest risk may not come from the coding changes themselves but from uneven organizational response.
Health systems with mature auditing programs, strong CDI integration, and consistent coding governance will likely adapt relatively quickly.
Organizations with fragmented workflows, inconsistent education practices, or overreliance on automated coding recommendations may experience wider variability in coding outcomes.
The most immediate priorities should include:
Focused auditing of high-variability categories, such as hypertensive emergency and secondary glaucoma
Education around newly permissible diagnosis combinations
Validation of encoder and grouper functionality
Alignment between coding, CDI, compliance, and revenue integrity teams
Increased review of documentation sufficiency for concurrent condition reporting
The danger is not a dramatic overnight disruption. It is the gradual accumulation of inconsistencies across thousands of encounters.
A Quiet Update With Long-Term Consequences
The April 2026 ICD-10 revision is a reminder that healthcare reimbursement systems do not need sweeping reform to create operational consequences.
Sometimes the most impactful changes are the least visible.
By loosening embedded sequencing hierarchy, expanding allowable diagnosis relationships, and increasing procedural specificity, the update subtly changes how coding decisions are made across the enterprise.
That shift places greater pressure on judgment, governance, and the integrity of documentation at a time when healthcare organizations are already balancing financial strain and operational complexity. The organizations that recognize the significance early will be better positioned to maintain coding consistency, compliance stability, and reimbursement accuracy.
Those who treat this as a routine update may discover the real impact only after denials, audits, and DRG variation begin to surface.
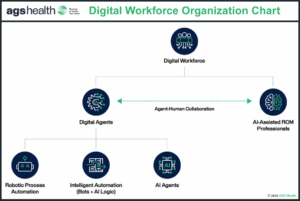
Healthcare providers are under unprecedented strain from rising claim denials, staffing shortages, and mounting margin pressures. To help meet these challenges, AGS Health, a leading provider of tech-enabled RCM solutions and a strategic growth partner to healthcare providers across the U.S., has introduced a new suite of agentic digital workforce solutions powered by AI agents and intelligent automation.
“Labor-intensive processes, fragmented RCM ecosystems, and continuously shifting payer rules have put healthcare finance leaders at a disadvantage,” said Patrice Wolfe, CEO of AGS Health. “CFOs are now dealing with alarming denial trends and significant financial threats that demand new strategies led by a collaborative digital RCM workforce built for scalability and engineered for impact. Through agentic AI, AGS Health empowers healthcare leaders with digital agents that work alongside their teams, taking on autonomous tasks and recommending data-driven next steps to improve decision-making.”
83% of organizations saw claim denials reduced by at least 10%.
68% reported improved net collections.
39% saw cash flow increase by more than 10%.
A New Class of Digital RCM Workforce
“AGS Health is answering the call for change with AI agents that level the playing field for overburdened RCM teams,” said Thomas Thatapudi, CIO of AGS Health. “Our next-generation, AI-infused workforce solutions bring speed, agility, accuracy, and human-like decision-making to critical RCM functions such as eligibility verification, prior authorizations, denials management, and appeals.”
AGS Health was recently recognized with a UiPath AI25 Award for its pioneering use of agentic AI to help healthcare organizations reduce the financial impact of denials. Its digital workforce features AI agents that understand natural language, adapt to changing rules and workflows, and make autonomous decisions to drive measurable business outcomes, including fewer denials and higher clean claim rates.
Key benefits include:
Financial: Faster reimbursement and lower cost-to-collect
Operational: Improved staff efficiency and focus on high-value work
Quality: Fewer errors in coding, data entry, and appeals
The Hybrid Intelligence Advantage
While AI systems can act autonomously, RCM professionals remain central to a successful digital workforce model. Skilled specialists help train and refine the AI, driving strategy while maintaining oversight and accountability.
“Our hybrid intelligence model combines AI’s speed, accuracy, and scalability with human expertise and empathy,” added Thatapudi. “AI agents manage high-volume tasks while professionals handle exceptions and guide continuous improvement. This can be achieved in-house domestically or through our globally distributed workforce model to reduce operating costs and allow for 24/7 production schedules.”
By preparing work, surfacing insights, and managing exceptions, AGS Health’s AI agents empower RCM teams to make smarter, faster decisions without compromising quality.
By Emily Bonham, senior vice president of product management, AGS Health.
In healthcare revenue cycle management (RCM), we’ve long relied on automation systems that process rules-based workflows with limited or no need for complex logic and nuanced judgement. Robotic Process Automation (RPA) has been highly effective at automating repetitive, high-volume tasks such as claim status checks and data entry.
However, its limitations are increasingly apparent. Today’s revenue cycle challenges demand more than just speed and efficiency; they require adaptability, context, and intelligent decision-making.
That’s where agentic AI comes in.
Agentic AI represents a next-generation approach to automation—one that mimics how humans think, make decisions, and interact with systems and people. Unlike RPA, which follows strict, predefined scripts, agentic AI models operate as autonomous agents. They’re context-aware, goal-oriented, and capable of reasoning across complex workflows. For revenue cycle teams under pressure from rising denials, staffing shortages, and shrinking margins, this kind of intelligence isn’t just nice to have—it’s becoming essential.
What Makes Agentic AI Different?
The simplest way to explain agentic AI is to compare it to a seasoned team member—one who not only knows how to complete a task but also when to escalate, adapt, or reprioritize based on changing circumstances. Agentic systems can:
Interpret and act on real-time data from multiple sources
Make decisions without human intervention
Learn from patterns and improve over time
Collaborate with human team members when needed
In practical terms, this means AI can now triage claims, initiate and complete payer calls, route work dynamically, or even autonomously document and code encounters—all with logic and consistency.
Why This Matters for RCM
Healthcare RCM is a perfect candidate for agentic automation because it sits at the intersection of structure and unpredictability. Processes are highly regulated, but real-world conditions vary constantly. Consider these examples:
Accounts receivable: Agentic AI can identify which claims require expert attention and which can be resolved through automation, ensuring staff spend their time where it’s most needed.
Insurance follow-ups: AI agents can navigate payer phone trees, wait on hold, retrieve claim information, and even update the EHR, without tying up human resources.
Denial management: Instead of flagging a denied claim for review, an agentic system can analyze the denial reason, check documentation, and suggest or initiate corrective actions.
These aren’t distant possibilities—they’re already being piloted and implemented in real-world environments.
The Human + Agentic AI Model
It’s important to note that agentic AI is not about replacing people—it’s about augmenting them. The most effective models combine human oversight with AI execution:
Human experts oversee automated workflows, handle edge cases, make nuanced judgment calls, or perform relationship-driven tasks.
AI agents handle high-volume, rule-governed, or low-dollar work with consistency and speed, while equipping staff members with insights and suggested actions.
This hybrid approach doesn’t just improve throughput; it also enhances job satisfaction for teams that no longer spend their days on tedious follow-ups or simple reconciliations.
Getting Started with Agentic AI
For organizations beginning to explore this space, here are a few guiding steps:
Consolidate and clean your data: Fragmented data across EHRs, billing systems, and vendor platforms limits AI effectiveness. Start by creating interoperable, governed data environments.
Identify high-ROI use cases: Look for repeatable processes with moderate complexity and clear financial upside, like denial prediction, prior authorization automation, or A/R follow-ups.
Experiment with short feedback loops: Choose pilots where you can quickly assess ROI and adjust based on results. Don’t aim for perfection—aim for momentum.
Build trust through transparency: Ensure your AI systems are auditable and explainable, especially when financial decisions are being made autonomously.
A Path to Sustainable Margins
Every healthcare leader is being asked to do more with less: deliver care, navigate compliance, and protect financial performance. Those who lead with tech-forward cultures by embracing intelligent automation and prioritizing data cleanliness in their revenue cycle operations are well-positioned to rise to the occasion. In contrast, those who resist innovation due to skepticism or overly protective and risk-averse policies risk falling behind—exposing their financial performance to volatility and long-term disruption.
Agentic AI offers a path forward, not as a magic bullet, but as a powerful tool for reclaiming time, improving accuracy, and aligning resources where they have the most impact.
It’s still early days for agentic AI in healthcare RCM, but the direction is clear. With the right balance of vision and pragmatism, revenue cycle leaders can unlock a new level of operational intelligence and move closer to sustainable, value-driven performance.
In 2018, the head of the Centers for Medicare and Medicaid Services issued a challenge to health IT developers and providers alike to “help make every doctor’s office in America a fax-free zone by 2020.”
The challenge was issued out of frustration with a vital workflow that remains reliant on outdated fax technology. Each year, healthcare providers exchange over 9 billion fax pages, driving an estimated $125 billion in costs across the healthcare system.
The continued reliance on fax technology is a persistent challenge for healthcare, undermining data integrity and operational efficiency. Studies by DirectTrust reveal alarming statistics: 30% of tests must be re-ordered due to lost faxes, and 25% fail to arrive on time for patient visits. Additionally, integrating faxes into health systems often demands manual indexing—an expensive and time-intensive task many organizations can ill afford.
Fortunately, automation offers a solution. Machine Learning and Generative AI are particularly adept at handling repetitive tasks such as fax indexing. While achieving perfect accuracy from the outset is unlikely, pairing AI-driven Digital Workers with human oversight ensures exceptions are managed effectively. Over time, as AI systems learn and adapt, they can assume more complex responsibilities.
To succeed, this model requires a carefully designed workflow that balances human expertise with AI capabilities to meet quality, timeliness, and accuracy standards.
Building the Digital Workforce
A successful hybrid fax indexing strategy relies on a carefully designed digital workflow model that effectively coordinates efforts between human staff and Digital Workers. The process begins with identifying the necessary technologies, which is best accomplished by observing human indexers to gain a comprehensive understanding of their workflows and unique requirements. This insight informs both implementation planning and feasibility testing.
By Ryan Chapin, executive director of strategic solutions, and Vijaya Krishna Veeravalli, senior vice president of cloud engineering, AGS Health.
Ryan chapin
As we head into 2025, several key trends are expected to significantly shape the future of healthcare revenue cycle management (RCM). From managing surging denial rates and evolving workforce dynamics to mitigating rising cybersecurity risks and integrating cutting-edge technologies, healthcare organizations are entering the new year while navigating a complex—often contentious—environment to enhance patient care and operational efficiency.
Navigating an Adverse RCM Environment
Denials, evolving payer relationships, and greater administrative burdens have come together to create what may best be described as an adverse RCM environment for healthcare organizations.
Climbing denial rates, prior authorization requirements, and the costs associated with managing both are among the most significant challenges confronting healthcare organizations going into 2025. According to an American Medical Association (AMA) survey, physicians reported spending nearly two business days per week completing an average of 43 prior authorizations—many of which end in denial.
Vijaya Krishna Veeravalli
In terms of denials, the surge is driven in large part by the growth in commercial and government third-party audits, including an increase in the volume of prepayment audits. According to MDaudit, external audit volume more than doubled between 2023 and 2024 and total at-risk dollars increased fivefold. The result was a sharp uptick in final denial dollars across professional (34%), hospital outpatient (84%), and hospital inpatient (148%) settings.
Healthcare providers participating in increasingly popular Medicare Advantage (MA) plans have been especially hard-hit. MDaudit reports that MA-related denials increased by 59% on average across professional and hospital settings in 2024, and the total denials amount for MA plans rose by 51%—a trend that has a growing number of providers reconsidering or dropping participation based on high denial rates and poor payments.
The impact of these trends goes deeper than financial. They add to already high administrative demands that in turn increase the strain on an overburdened—and increasingly costly—workforce that RCM leaders struggle to shore up in a tough recruitment and retention environment. To avoid staff burnout, healthcare leaders are continuing to adapt strategically, including exploring onshore, nearshore, and offshore outsourcing models.
AGS Health, a leading provider of tech-enabled revenue cycle management (RCM) solutions and a strategic growth partner to healthcare providers across the U.S., has received a UiPath AI25 Award for the company’s innovative use of automation and AI to support greater accuracy and efficiency in the intake and management of faxed documents.
Despite efforts to eliminate faxing, use of this cumbersome, inefficient, and costly technology by healthcare organizations remains prolific. Over 9 billion fax pages are exchanged annually at a cost of $125 billion, significantly straining already limited resources.
AGS Health’s IntelligentFax Processor automates this process, accelerating indexing, enhancing accuracy, reducing costs, and improving efficiency by leveraging a hybrid workflow model combining GenAI and robotic process automation (RPA) with manual indexers to handle exceptions. The system can handle a wide array of document formats and types, including consultation notes, test results, and medical records. Powered by advanced AI, it learns and adapts to the unique fax templates of each organization, ensuring accurate data extraction and categorization.
The annual UiPath AI25 Awards recognize the 25 most innovative UiPath customers using a combination of AI and automation as a strategic change enabler to accelerate bigger and bolder outcomes. AI and automation are redefining what’s possible—not just in business, but in the ways we work and live. This powerful combination creates fast, comprehensive, and actionable insights to inform decisions—uncovering never-before-seen opportunities for productivity and innovation.
Various forms of automation have long been present within healthcare revenue cycle management (RCM). However, advances in artificial intelligence (AI) have brought the industry to a significant inflection point, where the use cases for AI tools are expanding as rapidly as their capabilities.
We sat down with Thomas Thatapudi, chief information officer of AGS Health, to discuss the current and future state of AI in RCM and what healthcare organizations need to know about effectively integrating it into workflows.
EHR: How are automation and AI reshaping healthcare’s approach to revenue cycle management?
Thatapudi: Healthcare finance leaders have long recognized the power of simple automation, like simple rules-based workflows or analytics dashboards, to improve billing processes and error rates. Now, advanced AI tools like ChatGPT, large language models, and generative AI – or GenAI – have brought RCM to an inflection point with a variety of viable new AI-driven RCM use cases that could have significant financial impacts. AI and automation can reduce manual labor costs and increase net revenue through a seamless process that follows the entire patient journey, from preventing authorization denials upfront and reducing coding errors to implementing more proactive and efficient accounts receivable follow-up processes.
With front-end revenue cycle tasks such as insurance verification and prior authorization, we have an opportunity to create a completely seamless and interactive process for patients while ensuring the presence of appropriate controls to mitigate revenue leakage. For mid-cycle coding, certain specialties lend themselves to autonomous coding that eliminates the need for human intervention, freeing staff to focus on more complex work. On the back end, the focus can shift to denial management and collection rates, particularly for claims that, due to capacity constraints, were left unworked in the past. This can be particularly beneficial in cases where payer requirements have become more stringent.
These examples are just the tip of the iceberg in terms of potential RCM use cases over the next two years.
EHR: What are some examples of areas where AI tools are being used to improve RCM?
Thatapudi: AI is being used in clinical documentation, patient communication and payments, scheduling, prior authorization, and medical coding. In fact, coding has been utilizing true AI and machine learning in the form of NLP-based computer-assisted coding (CAC) for about a decade. With existing CAC applications reaching a plateau in coding accuracies of approximately 70-75 percent, new autonomous solutions are entering the market that leverage deep learning models and Gen AI to truly increase fully automated coding rates. I expect that coding will be one of the RCM areas that will be most heavily impacted by true AI, machine learning, and deep learning.
EHR: How can finance leaders make use of advanced data analytics and business intelligence (BI) tools to inform RCM decisions and measure their impact?
Thatapudi: BI tools can measure a wide range of metrics, from the number of system users to interactions and accounts, all of which can inform the key performance indicators (KPIs) that are crucial for monitoring financial performance. The problem is that the sheer volume of metrics can easily be overwhelming, which can lead to analysis paralysis. To prevent this, it’s important to take a step back and home in on KPIs such as financial indicators like collection rates per day or per month and the time it takes to collect payments—performance indicators that tell how much in time and money is being spent to recover a dollar so it can be reduced or better managed.
It’s important that senior leadership avoid being overly impressed by the wealth of intelligence that can be collected and displayed on a dashboard. The focus should instead be on determining the KPIs that drive day-to-day operational decisions. For example, predictive analytics services help healthcare organizations better predict denials, anticipate underpayments, forecast payments, and more. This allows for proactive claim correction prior to submission, which improves clean claim rates and cash flow. Creating simulations and projections for customized “what-if” scenarios provide an understanding of the impacts associated with interdependent metrics.


 Healthcare providers are under unprecedented strain from rising claim denials, staffing shortages, and mounting margin pressures. To help meet these challenges,
Healthcare providers are under unprecedented strain from rising claim denials, staffing shortages, and mounting margin pressures. To help meet these challenges, 
 y Thomas Thatapudi, CIO,
y Thomas Thatapudi, CIO, 


