The term “social determinants of health” is far more than a trendy new buzzword in health care. Serving the physical, mental and social needs of the community is not just the right thing to do but can mean substantial improvement in care and reduction in unnecessary healthcare costs.
Several studies have shown that addressing social needs, such as food or housing insecurity, can have a significant impact on a person’s healthcare outcomes and costs. Individuals experiencing housing insecurity or homelessness have higher rates of chronic diseases such as high blood pressure, heart disease, diabetes, asthma, chronic bronchitis, and HIV. This in turn leads to higher utilization of healthcare services such as emergency room visits, inpatient hospitalization and longer lengths of stay compared to those individuals with secure housing. Similar results are seen in those experiencing food insecurity.
Hospitals often state that part of their mission is to provide high quality care and improve the community’s health, or community benefit. A recent study of hospital mission statements in three states (Ohio, Florida and Texas) found that while quality was cited most often (65%), the second most frequently used term was community benefit (24%).[1] If community benefit or community health is part of your health system’s mission statement, how much are you really doing to address the whole health of a community vs. just addressing their “sickness” needs?
At PCCI, our combination of data scientists and expert clinicians believe that health systems have an obligation to address social determinants of health to ultimately remove the disparities and inequality that we see in our community’s health. Yet this is tricky because success requires outreach skills, community relationships and data insights that extend beyond the traditional promise of health-related services. That said, there are three key elements that can assist health systems in making an investment in social determinants of health a reality. To move from theory to action, my suggestion is that health systems do the following:
Leverage the board’s community presence to align on areas of greatest need
As part of health system leadership, board members ensure alignment between mission and a defined SDoH strategy at all levels of the organization. As community representatives themselves, board members can also create the momentum and connections that health systems need to bring community and business partners together to create a governance structure for launching a connected community of care. Such governance structure will guide the strategy, legal and policy needs, and the investment and execution of a connected and aligned SDoH strategy.
Invest in long-term partnerships to ensure sustainability
Recognize that as health systems, you alone cannot solve for social determinants. To truly meet the social, behavioral and emotional needs of some of the most vulnerable individuals in your community, you need to identify community partners with expertise in these areas. With the assistance of board members, assemble a partnership collaborative, with a formal governance structure, to build community-based strategies around SDoH needs. Support the sustainability of this collaborative with technology and data science techniques to identify specific root causes of social need in target populations, share data, and measure impact of interventions. Identify an independent partner to evaluate the effectively of the SDoH initiatives and measure the cost, savings and impact across the community and for the health system.
What is that one factor that separates one patient from another? Can one identify why two patients with the same illness but from different regions respond differently to a particular treatment? Do we need to cater to the needs of patients even after they leave the clinic?
These questions have always intrigued not only the physicians but every member who is involved in the care journey— care teams, communities, social workers, even patients themselves. And the answer lies in just one fact— even if these two patients appeared similar on paper, their lifestyles are very likely to differ: socioeconomic status, gender, race, ethnicity, family structure, and education.
All of this comes down to just one term: Social Determinants of Health.
This is one of the prime problems that has kept healthcare organizations in a situation of dilemma.
We are way past the statement that SDoH is just another hype
Have you ever tried to score a home run with one hand tied behind your back? This situation is similar to the condition of healthcare organizations in the value-based ecosystem. They are trying to get 100% of the task of healing a patient done with just 50% of the insights.
Social determinants matter because they can affect the health of the population residing in a particular region, for better or for worse. We have countless studies that show the importance of social determinants, yet we are not able to properly address them because we are not able to answer these questions:
How do we address the challenges that we don’t even know exist?
Who is responsible for addressing these challenges?
Is there any ideal strategy to address SDoH?
No matter how famous they are in healthcare, working with SDoH requires a drilled-down approach and something that we have in abundance- healthcare data. This data can be leveraged, and with the use of predictive analytics, organizations can accurately measure the at-risk population and advance preventive care methods in the ecosystem.
The best way, I think, is to look at this picture with a magnifying glass. Traditionally, the endpoint is the state-level analysis of SDoH. However, it is not the end but the beginning of the study that should go to the zip code level.
Here are some of the most interesting stories of how the leaders in the field of addressing the Social Determinants of Health addressed the populations’ needs and did the undoable.
What was the Humana way to deal with the non-clinical factors?
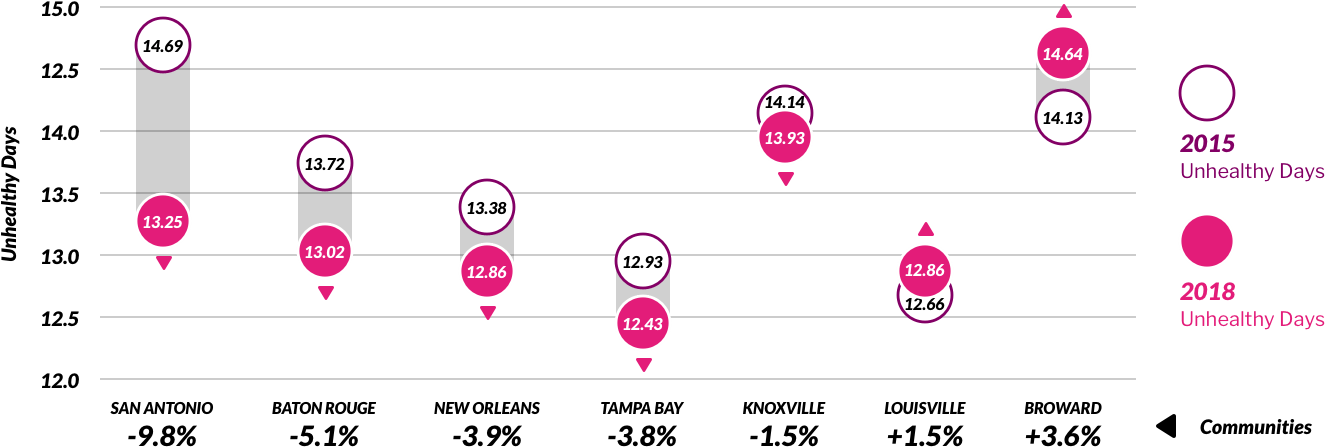
Humana has the Bold Goal Initiative, which is a population health strategy that is aimed at improving the health of the communities and making them 20% healthier by the year 2020. Their Healthy Days surveillance process is a robust and scalable metric. Based on this, they found that food insecurity and loneliness were among the top contributors to the total unhealthy days among the population they serve.
With their holistic and comprehensive approach, they built an analytic intervention pipeline to address these issues. One instance is their intervention with Papa Inc., where they connected college kids to seniors who needed companionship. As a result, 94% of members stated that the Papa Program helped them to feel more socially connected.
Humana was able to reduce the number of unhealthy days from 2015 to 2018 by simply addressing the non-clinical aspects of care delivery for their population.
Performance of Humana’s seven original Bold Goal communities (2015-2018) – Humana Medicare Advantage members
How MercyOne PHSO took the understanding of non-clinical factors from the zip code level to an individual patient level?
MercyOne PHSO, one of the largest ACOs in the Midwest, wanted to know the factors affecting their patients. They took the simple concept of asking the right questions and leveraged it to understand their patients.
While their patients entered the hospital or examination room, they asked them to complete a survey consisting of questions that depict the factors that affect their patients’ health, such as:
In the last 12 months, were you worried that your food would run out before you got money to buy more?
What is your living conditions today?
Do you face any difficulty in reaching out to your doctor?
Health Level Seven International (HL7), the global authority for interoperability in health information technology, and the American Academy of Family Physicians (AAFP), the only medical society devoted solely to primary care, are pleased to announce that the Gravity Project is now part of the HL7 FHIR Accelerator Program.
The Gravity Project aims to standardize medical codes to facilitate the use of social determinants of health-related data in patient care, care coordination between the health and human services sectors, population health management, value-based payment and clinical research. Social determinants of health (SDOH) are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.
The HL7 FHIR Accelerator Program is designed to assist implementers across the health care spectrum to create HL7 FHIR implementation guides and other products than can facilitate FHIR acceleration and adoption activities. Other projects within the Accelerator Program include Argonaut, Da Vinci and CARIN Alliance.
Why the Gravity Project? Unmet social needs including limited access to food, transportation and housing can negatively impact health outcomes. Research has demonstrated that addressing social and medical needs in tandem improves health outcomes and lowers costs.
“Progress in patient care and research has made significant strides with the emergence of the HL7 FHIR Accelerator Program,” said HL7 International CEO Charles Jaffe, MD, PhD. “By incorporating the social determinants of health care into our decision process, the Gravity Project will help to transform care delivery and health analytics.”
In this context of mounting interest around collecting and using SDoH data in healthcare settings, new challenges have emerged related to the capacity of existing medical terminology standards to effectively capture, use and exchange the necessary data.
The Social Interventions Research and Evaluation Network (SIREN) at the Center for Health and Community, University of California, San Francisco, was an early catalyst of the Gravity Project, convening a diverse group of stakeholders as early as November 2017 to develop a strategy for achieving consensus-based comprehensive coding standards for SDOH data capture in EHR systems.
“With funding from the Robert Wood Johnson Foundation and in partnership with EMI Advisors LLC, SIREN is pleased to be working with multiple stakeholders to meet the rapidly expanding market needs around SDOH data documentation and interoperability,” said SIREN Director and UCSF associate professor of Family and Community Medicine, Laura Gottlieb, MD, MPH. “Building on work originally supported by Kaiser Permanente and the Robert Wood Johnson Foundation, the Gravity Project’s new partnership with HL7 will strengthen the capacity for SDOH information exchange between stakeholders, including clinical providers, patients, community organizations and payers.”
The Gravity Project has established a public collaborative process initially focused on three domains: food security, housing stability and quality, and transportation access. The project is working to:
Develop use cases to support documentation for screening, diagnosis, treatment/intervention, and planning activities within EHR and related systems;
Identify common data elements and their associated value sets to support the uses cases;
Develop a consensus-based set of recommendations on how best to capture and group these data elements for interoperable electronic exchange and aggregation; and
Develop an HL7 Fast Health Interoperability Resource (FHIR) Implementation Guide based on the defined use cases and associated data sets.
“The AAFP is pleased to act as convener for the Gravity Project and support information interoperability efforts,” said Shawn Martin, senior vice president of advocacy, practice advancement and policy for the American Academy of Family Physicians. “Our vision is to transform health care by addressing the social determinants of health through efforts such as our innovative HealthLandscape geoanalytics platform and The EveryONE Project to help family physicians take action and confront health disparities head-on. The important work of the Gravity Project will advance data exchange and allow family physicians to better care for patients and communities.”
The Blue Cross Blue Shield Association (BCBSA) is an active member of HL7’s initiatives to advance interoperability, and has joined SIREN and AmeriHealth Caritas in co-sponsoring the Gravity Project launch. Additionally, both the BCBS System and AmeriHealth Caritas have several programs in place to address SDOH, including actively collecting SDOH health data, engaging community health workers, providing rides to doctor appointments, and delivering healthy, affordable meals to people’s homes.
“The social and environmental conditions in which we live, such as access to healthy food and housing or reliable transportation, are critical to our health,” said Dr. Trent Haywood, chief medical officer for BCBSA and president of the Blue Cross Blue Shield Institute. “The Gravity Project will help enable the data interoperability that allows the entire health care community to address barriers that limit the ability to achieve optimal health.”
The Gravity Project has convened more than 500 experts from across the nation including clinical and community-based provider groups and payers to health technology developers and standards stewards, to collaboratively develop recommendations for how best to capture data about food, housing, and transportation risks and needs, for interoperable electronic health information exchange.
“AmeriHealth Caritas has been actively collecting social determinants of health data from member households for the past two years to help us better address their needs,” said Andrea Gelzer, MD, senior vice president of medical affairs for AmeriHealth Caritas. “The Gravity Project affirms our collective belief that standardizing the ways in which we all collect data will enable providers, plans, and other supportive agencies to quickly and more strategically mobilize care for the populations we serve.”
Participation in the Gravity Project is open to all interested organizations and individuals.
“We are pleased to coordinate and facilitate an open, transparent, and virtual community via the HL7 suite of collaboration tools,” said Evelyn Gallego, MBA, MPH, CPHIMS, program manager for the Gravity Project, and EMI Advisors CEO. “We invite all interested parties to visit the HL7 Confluence page to learn more about the Gravity Project, including how to become a participant and/or a sponsor of this important endeavor.”
AdhereHealth has announced a partnership with Papa, a companionship platform company serving the elderly, blind and disabled. A growing issue for millions of Americans enrolled in Medicare are SDoH, such as loneliness, food insecurity and transportation, any one of them impeding optimal healthcare and medication adherence. This combined relationship addresses foundational barriers to care through advanced technologies and a compassionate, personal interaction.
“We could not be more excited about this
partnership as it extends the Adhere platform’s reach into the home with Papa
assisting those most in need of personal support,” said Jason Z. Rose,
AdhereHealth CEO. “Our analytics and clinical workflows will help direct Papa
Pals to address a myriad of SDOH issues our consumers face, such as
transportation to doctor appointments and local pharmacies, grocery shopping,
housing chores, and other senior services.”
In 2018, CMS announced
a new policy allowing Medicare Advantage and Part D health plans to pay for
SDOH services as a medical expense for seniors with chronic diseases. Now
AdhereHealth can deploy “Papa Pals” to consumers at risk for poor health
outcomes for face-to-face support. Most Papa Pals are college students
majoring in nursing, social work, or hospitality that desire to improve
consumer quality of life.
Andrew Parker, founder and CEO of Papa, shared,
“We have realized that social determinants of health in America is an
increasing factor in medical non-compliance.” He continued,
“Collaborating with AdhereHealth will allow Papa’s team of personal
companions to make an intergenerational impact on the most vulnerable in our
society, providing them the freedom to age in place while having an advocate at
their side to aid them in the journey through health care.”
Graduating from Silicon Valley’s prestigious Y
Combinator accelerator program, Papa works with large Medicaid and Medicare
clients who have embraced companion health for their members. The Centers for
Disease Control and Prevention uses the healthy days metric to measure consumer
quality of life. This partnership is immediately available to over 20 million
American’s covered by Medicare Advantage plans, plans interested can visit www.adherehealth.com/papa.
At this point, most of us in healthcare have read similar statistics about why we need to do more to address social determinants of health (SDoH) — the conditions in which people are born, grow, live, work and age, and how those factors impact individuals’ health — to improve patient outcomes. These conditions and their resulting social needs include, but are not limited to, a person’s equitable access to nutrition, housing, transportation, education, and employment opportunities.
Time is of the essence to tackle some of these social determinants, especially when coupled with the rapidly shifting patient demographic, sometimes called the “silver tsunami.”
Payer
SDoH studies in no short supply
It seems everyone is in a race to figure out what SDoH approach will move the needle toward lower risk for their patient populations. But payers, in particular, have taken on a hefty amount of the leg work needed with social determinant “barriers to care” studies, because they are generally the most financially accountable, from a population health analytics perspective, to remove them.
Recent news about of these payer SDoH pilot programs and research studies have been both interesting and useful across the care continuum, a summary of which include:
WellCare, which provides managed care plans for over 4.4 million Americans, ran a pilot program on over 33,000 patients, referring them to more than 100,000 community-based social services programs, and was able to reduce inpatient spending by 53%, outpatient spending by 23%, and emergency spending by 26%.
In its Bold Goal 2019 Progress Report, Humana focused on patients in specific lines of business, including their Medicare Advantage program, where 91% of seniors who have at least one chronic condition. They enacted the Centers for Disease Control and Prevention’s “Healthy Days” self-reporting method of measuring healthy vs. unhealthy days and have also screened half a million people for SDoH since 2018, with the goal to screen one million by 2019. Humana notes that these social barriers are “deeply personal,” which requires closer partnership to track and measure population health.
Blue Cross is already instituting food, nutrition, and housing services as part of some of its plans. But it also recently announced an investment of $40 million with Solera Health, to address both mental health and SDoH matters, including “food insecurity, medically tailored meals, transportation, falls prevention, and social isolation” with lifestyle modification programs such as diabetes or management, and tobacco cessation programs.
A study by the Anthem Public Policy Institute says individuals and the public (researchers and journalists) perceive SDoH differently. Individuals tend to lead with concerns about the health care “system,” whether they can find the right provider, followed by whether they have adequate “social support.” The public tends to “frame health outcomes through the lens of structural factors like education and income level perhaps, in part, because these factors are easier to measure.”
UnitedHealthcare and the American Medical Association partnered to expand the existing ICD-10 diagnostic codes being used to identify social and economic barriers to care. This adds 23 more codes to that list, some of which would “indicate a patient’s inability to pay for prescriptions, inadequate social interaction, or fears about losing housing.”
Existing
workflows provide best locale for SDoH communication
Despite all of the various innovative steps being taken to bring SDoH to the forefront, we know that most patients still aren’t talking about SDoH concerns with their physicians. There are many reasons why, but one logical solution to bolster SDoH communication between physicians and patients is to incorporate, at minimum, the ability to identify social needs where they are already doing business — in these EHR, CRM, and other third-party platforms.
As is evidenced by the silo’d health IT data systems that have for too long crippled the health care industry’s transparency and ROI, we know that simply identifying social barriers to care is not enough. Within the designated “source of truth” that is most responsible for driving patient engagement, whether that is an EHR, CRM, or other platform, we need to build — or integrate — expanded capabilities for SDoH identification, referrals, and tracking each throughout the continuum of care to close the gaps that currently exist.
That is not to say that physicians must now wear yet another hat — that of a social worker or a social services case manager. But being asked to solve SDoH from the current physician’s workflow perspective, without integrating SDoH into the patient record, is basically saying to physicians:
“Improve clinical outcomes. But first, you must identify non-clinical data, be responsible for referrals to improve these individual circumstances, and track each of those referrals’ progress, all in different platforms, and none of which talk to one another.”
This is not setting our patients or their physicians up for success.
The idea of a standardized SDoH screening mechanism within the EHR has been endorsed by the National Academy of Medicine, the Medicare Access and Children’s Health Information Program Reauthorization Act of 2015, the 2016 Centers for Medicare and Medicaid Services’ Quality Strategy, and several other organizations, as released in an Annals of Family Medicine study. But unfortunately, in this first U.S. study of its kind to address feasibility, “little is (currently) known about how to capture and present (SDoH) information in community health centers’ EHRs.” Nor did the study conclude how to integrate EHR-based documentation needs into community health centers’ existing workflows.
The main barriers cited in the Annals’ study were that EHR-based SDoH tools: (1) Create a too-fragmented view of the patient, with relevant data in too many disparate locations (2) Might add a layer of difficulty to obtain and act on SDoH data (3) If SDoH patient information has been acquired on paper, that requires yet another dual, manual data entry problem when “referral workflows were (already) seen as too time-consuming, especially when no follow-up was planned,” resulting in “an unmanageable follow-up workload.”
To date, the EHR has done a good job of serving most of the goals to take our country’s health records digital. But it is also safe to say that the EHR, in and of itself, cannot be all things to all persons working in health care. In addition to the major enterprise EHR systems, there is a proliferation of specialty, industry-specific EHRs, which may or may not have separate CRM platforms, not to mention all of the other third-party, various other platforms you can see within any one given practice, such as separate billing and referral management types of platforms. There is a reason that “interoperability” among all of these disparate health care data systems has become another hot topic for the industry.
To yield maximum value for our customers, integrating SDoH data is best-approached from a workflows perspective — not just connecting disparate data systems for the sake of “more data,” but to make caregivers’ lives easier, and to create actionable data that enable better business decisions. And we already know that one of the easiest ways to improve efficiency for health care organizations is to remove dual, manual entry between EHR, CRM, and other third-party platforms that hold patient data — these are the first and most valid case studies of how to improve organizational efficiency while bolstering patient care.
There has been a flurry of innovative partnerships and technological improvements to address SDoH, all of which should ultimately be supported by policy changes — each of these as prevailing themes at trade shows and conferences in recent years, such as the America’s Health Insurance Plans’ (AHIP) annual conference, held recently in Nashville. Meanwhile, we look forward to participating in more discussions about how those of us in health IT can do our part — bridging SDoH informational and communication gaps between physicians and patients. This could include integrating non-clinical SDoH concerns into the patient’s clinical record, in and out of these platforms, establishing standards for capturing SDoH to make data-sharing easier, and even incorporating social services databases for more streamlined SDoH-specific “referral management.”
We talk a lot about how to achieve interoperability in healthcare, with all of its disparate data systems, and SDoH is another compelling and recent reason why we must accelerate these solutions, which would ultimately benefit health care and all of its stakeholders — patients, physicians, payers, and everyone in between.
By Hants Williams, director of clinical operations, VirtualHealth.
Hants Williams (Photo by Marcela Nowak)
The buzz around social determinants of health (SDoH) is making waves across the healthcare industry. Linked to roughly 80 percent of overall health, stakeholders are increasingly embracing the opportunity of addressing SDoH in care management workflows.
SDoH are defined by Healthy People 2020 as the “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning and quality-of-life outcomes and risks.” Essentially, these elements encompass the non-clinical factors that can promote or hinder a patient’s ability to fully comply with care plans.
Transportation sits at the heart of current SDoH initiatives as a fundamental prerequisite to optimal care. Simply put, if patients cannot pick up their medications or get to appointments, a provider’s ability to impact their patient’s health is minimized. Consider, for example, a recent Connance survey that links 50 percent of re-admissions to factors such as transportation and home instability risk.
In the era of value-based care, the simple act of helping patients access transportation can notably improve the outlook on clinical outcomes and costs. For instance, medication adherence is a focal point of industry efforts to improve clinical outcomes, but if a patient cannot access transportation to pick up needed drugs, the potential for improvement is minimized.
Access to transportation is low-hanging fruit in terms of performance improvement, and providers must get ahead of the transportation challenge to implement successful, sustainable population health strategies. It’s also why forward-looking organizations are addressing this critical element of SDoH by equipping care managers with tools that speed identification of transportation needs and available services.
Understanding the Challenge; Recognizing the Opportunity
Industry statistics reveal that the transportation challenge is significant and is expected to compound in the coming years. Estimates point to 3.6 million Americans missing or delaying medical care because of an inability to get to their appointments.
Understandably, the transportation issue is exacerbated in low-income and elderly populations as well as rural regions where public transportation is scarce. Many patients simply lack the disposable income needed to maintain a reliable source of transportation. In terms of elderly populations or those with disabilities, physical or mental conditions that eliminate or significantly restrict driving as an option create additional challenges.
The current and coming transportation challenge is sizeable and will require significant resources. Fortunately, the business case for improving the outlook is an easy one to make: A recent study examining non-emergency transportation costs in Florida found that if a mere 1 percent of medical trips resulted in the avoidance of an emergency room visit, the state could save up to $11 for each dollar spent.
Advancing Transportation Strategies
Providers and payers alike are increasingly turning to tools that help identify SDoH needs like transportation in near real-time, allowing care managers to proactively seek out community resources that can help. For example, one state-run managed Medicaid program deployed a care management platform that allows clinical teams to access pre-approved community services and schedule transportation appointments immediately once needs are identified.
With the help of customized algorithms and advanced artificial intelligence tools, drivers can be deployed to patients’ homes in anticipation of needs rather than finding out after the fact that appointments were missed, or medications were not picked up. The efficiency of the analytics platform is critical to changing the dynamic as clinical teams would otherwise be tasked with combing through millions of line items in patient records to identify potential needs.
Advanced solutions allow users to easily monitor transportation requests across all patients or drill down into a single case to manage unique details of each trip, such as advanced authorizations or ensuring the appropriate vehicle has been scheduled to accommodate assistive devices, child seats and companions. Care managers improve efficiency by scheduling recurring trips and tracking specific patient requests or preferences, which can be shared with the transportation vendor and other care coordinators.
Leveraging the transportation functionality, the state-run Medicaid program completed nearly 24,000 transportation entries in 2018. Through advanced analysis, it was able to forecast usage trends across months, time of day and geography to help its clients optimize operations and predict transportation expenditures. For example, the organization can determine which patients are frequent transportation users, which can alert care managers to book multiple provider appointments at once to reduce costs versus on separate days.
Personalized care management and coordination is part of the healthcare industry’s overarching goal of cultivating healthier communities. SDoH indicators such as transportation are critical to these efforts. Forward-thinking organizations are taking hold of the opportunity to improve care management by investing in infrastructures that support greater access to transportation.
By Abhinav Shashank, CEO and co-founder, Innovaccer.
Abhinav Shashank
Once while I was scrolling through the news feed on my phone, there was one specific line that really made me wonder: “There’s a 40 percent chance of gusty and blustery winds today.” Statements such as this one strongly influence people’s behavior, as they are based on evidence or data findings from years of surveying, studying, and analyzing past trends and occurrences. However, my question is “Why are we not able to make such claims in healthcare- even today?”
Can we predict the vulnerabilities a patient might face in the future or the current health risks a population segment faces?
Is risk scoring the answer we have been looking for?
Almost all kinds of care organizations have some risk scoring methodology to target care interventions. With quality, costs, and patient experience taking the center stage in healthcare, care organizations need to stratify patients based on their need for immediate intervention.
The need of the hour is to address high-risk issues that impact large groups of patients and ensure that these needs are met in a timely fashion. Often, frequent fliers among high-risk patients come into the emergency department as if it’s their second home.
What if we take the method of risk scoring to a whole new level?
Traditionally, providers and health systems have relied on claims-based risk models, such as CMS-HCC, ACG and DxCG, which were built to forecast the risk of populations/sub-populations but not for individual patients. Hence, these models give an accurate prediction of the average risk of the population but exhibit very poor accuracy if used to predict risk for individual patients.
Although risk scoring has turned out to be a key factor in addressing the needs of the patient population, this method cannot provide all the important insights that are needed to drive necessary interventions. Since healthcare already has the right data from sources such as EHRs, claims, labs, pharmacy, social determinants of health (SDoH) and others, can we predict the future cost of care instead of just stating the risk score of the patient?
The right machine learning-driven approach to predict the future cost of care for patients
It all starts with the right data. The first step is to integrate the data from multiple sources- whether it is clinical or non-clinical data, such as SDoH. The data from these sources can allow us to use the comprehensive patient’s data for multiple predictive models to predict future health cost with greater accuracy.
The reality is that very few people are doing great things with SDoH at this point. A lot of vendors and providers are thinking and talking about SDoH, but many of them don’t yet understand which social determinants are relevant or what to do about them. While the area is too new to boast a list of best practices, an introduction and discussion to the topic might be helpful for those considering a foray into SDoH.
What are SDoH?
The Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services, defines SDoH as “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.”
If you think that sounds broad, you’re absolutely right. These determinants cover everything from how clean your water is to what your friends are like. The factors are innumerable. Stakeholders estimate that only 20 percent of one’s health is based on clinical care received from healthcare providers, with another 20 percent to 30 percent based on genetics and at least 50 percent based on SDoH.
With those assessments in mind, it seems unfair that almost everything related to health is pinned on provider organizations. The healthcare system cannot be the only player. We say that it takes a village to raise a child, and it would take a village to adequately deal with social determinants.
But those working in healthcare can’t just wait for villages to get involved. As the market continues to shift toward value-based reimbursement, health systems, payers, and vendors will be expected to incorporate SDoH into their tools and patient care. A few principles might help these stakeholders to get started.
The beginnings of a SDoH strategy
An organization’s first step in incorporating SDoH into their strategy should be to decide which data is the most important. For example, it probably wouldn’t help a physician to know which university a diabetic patient attended, but it could help a lot to know that the patient orders takeout almost daily because he doesn’t have a car and isn’t within walking distance of a grocery store with healthy options. These are aspects that, one day, may fall under the banner of SDoH.
Once an organization knows which data elements they want, they can determine how to get it. Unfortunately, the regional nature of SDoH data makes creating an excellent database very difficult. This is why we need vendors to keep SDoH on their minds. Providers need their vendor partners to incorporate SDoH data into their EMRs, population health tools, and other platforms. Healthcare organizations can also gather data by conducting assessments on-site or at patients’ homes.

 Is there any ideal strategy to address SDoH?
Is there any ideal strategy to address SDoH?