By Beth Haenke Just, MBA, RHIA, FAHIMA, founder and CEO, and Karen Proffitt, MHIIM, RHIA, CHP, vice president of industry relations/CPO, Just Associates, Inc.
Beth Haenke Just
The introduction of overlays into a medical record system can be so subtle that they often go unnoticed until one causes an adverse event, HIPAA violation or billing error—making them a primary source of patient errors, expenses and lost revenues in hospitals today.
Caused when the information of two patients is co-mingled within one medical record, the dangers of overlays have intensified with the proliferation of electronic health record (EHR) systems, which accelerate the rate at which multiple internal and external systems can be infected with dirty data. Compounding the problem is an overreliance on technology-centric solutions to resolve possible duplicates.
The American Health Information Management Association (AHIMA) puts the average duplicate rate at between 8 percent and 12 percent. A more recent survey by Black Book found an average of 18 percent. Meanwhile, an analysis of EMPI cleanup projects Just Associates completed between 2012 and 2016 showed that as many as 1.3 percent of these possible duplicates are actually potential overlaid records.
Karen Proffitt
When it comes to overlays, there are three challenges facing health information management (HIM) professionals tasked with maintaining the integrity of patient records: 1) identifying and resolving existing overlaid records, 2) determining the root cause(s) and 3) implementing policies and procedures that will prevent the creation of new ones.
The birth of an overlay
The most common way an overlay is created happens at the time of registration when an incorrect patient record is selected, core demographic information is changed, and a new visit is added. Occasionally, the records of two different patients are erroneously merged during the duplicate resolution process.
Overlay creation can also be traced back to multiple departments. A study in the Journal of AHIMA involving an eight-hospital, multi-state healthcare organization found that most of the errors happened in the emergency department (ED) and, to a lesser extent, in registration, scheduling and ancillary areas such as lab and radiology.
The hospital system that was the subject of the study had been tracking and keeping detailed statistics on overlay errors for five years, beginning with the implementation of an EHR system. This provided researchers with the rare opportunity to analyze a considerable sample size of 555 errors, from which they determined an error rate of one in every 10,734 admissions. That is the equivalent to more than nine errors per month, of which 97.5 percent were caused by user oversight. The study also identified an upward trend in overlays attributed to growth of the health system and higher utilization of error identification tools that reveal more issues than manual methods.
For example, 54 percent of overlays were found by registration users while data integrity change reports that made use of EHR tools found 31 percent. Clinicians were a distant third, identifying just 6 percent of errors. Patients also found overlay errors via patient portals, which could have allowed them inappropriate access to highly-sensitive protected health information (PHI) — access that could lead to HIPAA violations.
Proactive EHR tools found most overlays within 10 days of their occurrence, and most were corrected in 30 days. This is important because the longer an overlay goes undetected, the less likely it will be found. When it is found, the older overlaid record is much more time-consuming and expensive to correct.
The high cost of overlays
To determine just how costly overlays are, it is necessary to cast a wide net, as few studies have been done to establish industry averages. Factors contributing to the full financial impact of an overlay include denied and delayed claims, lost revenues and resources required to identify and correct the error.
Time is a huge factor in the costs associated with overlay correction resources. For paper-based overlays, it can take between 60 and 100 hours, while EHR-based errors can take months depending upon system complexity. A survey by the College of Healthcare Information Management Executives (CHIME) further found that respondents typically had at least two people dedicated to “data cleansing,” including overlay correction.
Imagine for a second: you’re walking through the busy halls of your local hospital, only to notice that the doctors and nurses around you are constantly checking their phones and tablets. It strikes you as odd, and you can’t help but think: Isn’t anyone getting any work done around here?
Actually, they are.
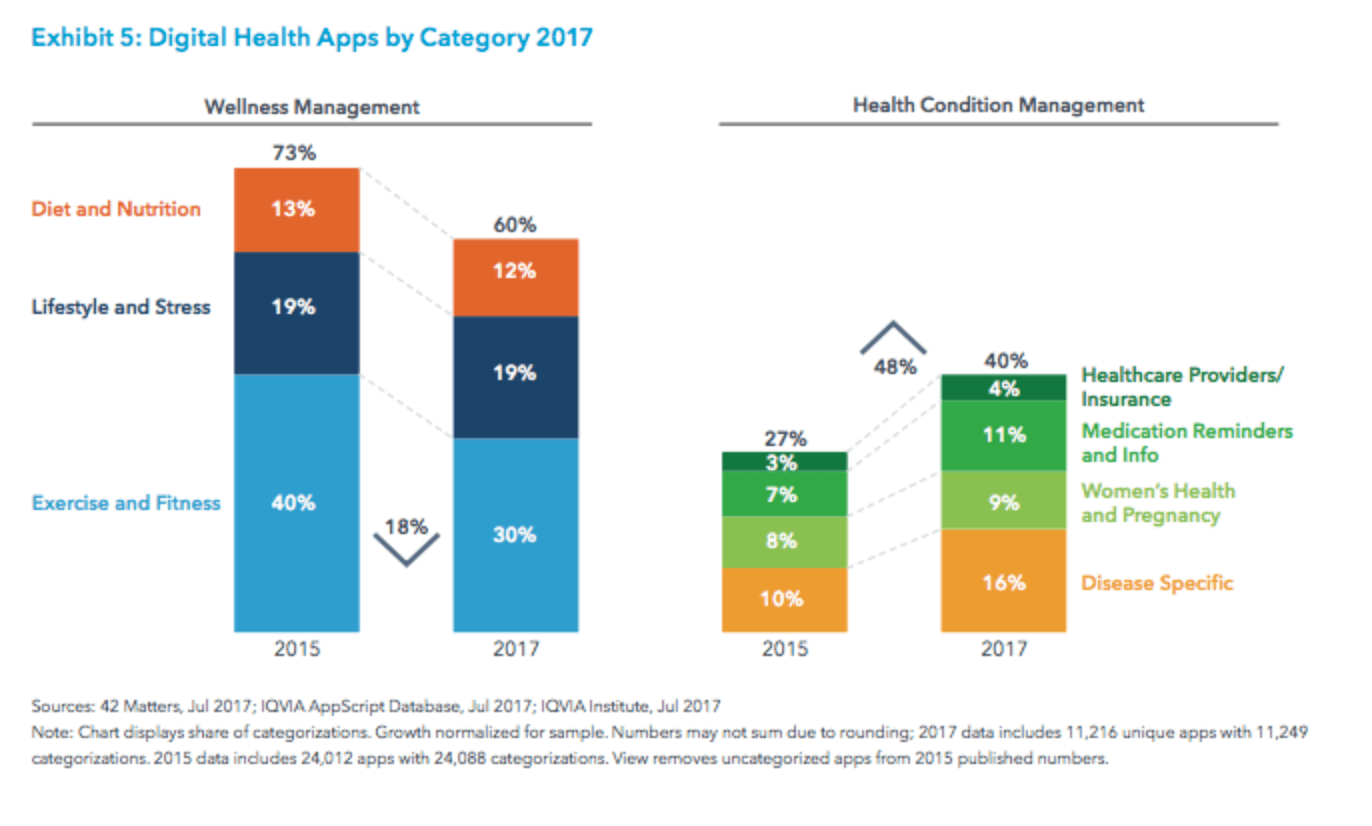
With over 70 percent of examined patients using at least one health app to manage their diagnosed condition, and more than 318,000 mobile healthcare apps available in top app stores worldwide, the picture of doctors and nurses relying on their devices as literal “mobile assistants” is becoming a highly sought-after reality.
While this perspective is often bolstered by positive reviews of hand-held computer use by healthcare professionals – where digital assistant devices improved physician effectiveness during patient documentation, patient care, information seeking and professional work patterns — the mHealth industry still has a lot of room to grow in terms of digital health infrastructure.
Not to be put off, mHealth developers have nevertheless continued to advance their compliance, security, accessibility, and efficiency practices in the face of wide-scale transformative change. And when asked, most mHealth developers (myself included) will tell you that what motivates us to keep going has to do with the massive potential these technologies have to literally transform the field of medicine as we know it.
And what exactly is thatpotential? Every day our news feeds are inundated with articles promoting the latest in mHealth technology – from mobile apps that can perform an ultrasound, to apps that help patients track their own symptoms – so it can be hard to navigate the ever-widening world of mobile healthcare.
In light of such a big subject then, I’ve often taken to cementing my own understanding of mobile health by thinking about the ways in which these applications are already affecting physicians, clinicians, and other practitioners at every stage of their medical career.
Put differently, from the time that an aspiring healthcare professional begins their educational journey, to their first-accepted payment for needed treatment, mobile health apps are helping doctors transform the field of medicine before our very eyes. Here’s how:
Medical Education
In a lot of our popular media, physician education is represented as an arduous journey from beginning to end. With long nights studying, cadavers to examine, and an infinite amount of medical information to digest, med students are flocking to (mobile) medical education applications that can help them test their own knowledge in a way that suits their learning style.
Medical billing is process of handling and managing claims, processing payments, and generating revenue. It entails various tasks – coding claims correctly, tracing them, following up and much more.
The medical billing task is challenging and demanding too. But, it can be made easy by integrating the billing system with an EHR software.
Let’s have a look at the integrated electronic health records benefits in medical billing process.
Improve efficiency
When the billing process is integrated with an EHR, it becomes a comprehensive platform. You don’t need to input the data manually and repeatedly.
The integrated system also removes the need to fax or photocopy every billing sheet. This not only saves time and boosts productivity, but also minimizes human error during data transfer, saves paper and money.
Enhance comprehensiveness
EHR becomes a comprehensive platform to perform a number of activities. Accessing data from a single place makes your process highly cost-effective and accurate.
Build trustworthy relationships
Integrating your EHR and the billing system brings in transparency in the medical billing process. The EHR software seamlessly integrates with billing system to submit cleaner claims and schedule appointments more easily.
In part, the article blames the shortage on the “graying” of America, as both medical professionals and patients age, stating that “one-third of active doctors will be older than 65 within the next decade.”
But our organization believes the impending shortage has much more to do with the state of health care today, which is causing doctors to leave the practice of medicine—or not enter the field in the first place. In fact, many physicians now discourage their own children from following in their footsteps.
The shortage is less about doctors with gray hair, it’s about what Congress, regulators and health plans have done to cause doctors to pull out their hair. As evidence, a separate recent study found that a majority of doctors say “barriers set by insurance plans have led to worsened conditions for patients in need of care.”
Researchers with Aimed Alliance found that doctors are so fed up with the constant headaches caused by insurers, two-thirds would recommend against pursuing a career in medicine, and nearly half (48%) are considering a career change altogether. Unfortunately for patients, every exiting physician takes decades of expertise and experience with them never to be used again for care and cure.
Another culprit is the mandated government-certified electronic health records (EHRs), which is forcing doctors to use a technology system that wasn’t made for patient care. The EHRs have been called clunky and cumbersome. Studies also show that physicians spend twice as much time tending to the computer as they spend tending to the patient.
Physician-staffing firm, EmCare, became the latest of several victims within the healthcare industry of an email phishing scam, as an unidentified hacker recently gained access to the accounts of multiple EmCare employees. The fallout was devastating: 60,000 people–more than half of which were patients–saw their personal information, such as names, birthdates, private clinical data and even Social Security numbers become compromised.
Company officials at EmCare have declined to provide specifics on when they first became aware of the email breach but offered that their focus going forward will be centered on “… providing impacted individuals information about the incident and guidance on how they can protect themselves.”
An alarming trend
The recent EmCare email breach is not an isolated incident within the healthcare industry. In fact, healthcare has become the most vulnerable industry for such incidents as the number of email data breaches in the last two years has witnessed a bigger increase in healthcare than in any other industry.
A recent article published on ModernHealthcare.com shows that the number of reported healthcare email breaches doubled between 2016 and 2017. While the number of incidents plateaued in 2018, the number of individual healthcare records that were exposed doubled from last year.
So why have healthcare providers become such a popular target among phishing hackers? While the financial industry is obviously “where the money’s at,” financial institutions have made it very easy for their customers to cancel and replace a stolen credit card. But you can’t just cancel and replace your social security number or other private information, and nowhere is such data more readily available to hackers than in healthcare records.
The problem
When you purchase a car, no one asks you if you’re going to get car insurance. It’s assumed that you will because it’s of vital importance. Yet for some reason, the same logic doesn’t apply to email security. Even for healthcare providers whose databases contain private information that if compromised, could place their patients in dire circumstances.
When we look at the healthcare industry over the past 15-20 years, it is clear that drastic improvements have been made because of technology. For example, neurologists can now assess patients experiencing symptoms of a stroke remotely, using a specialized computer system. Wearable devices can track a patient’s vital signs and heart rhythm, alerting both the patient and their care team should any warning signs appear.
Furthermore, technology deployed throughout hospitals and healthcare systems has steadily improved the efficiency of caregivers and allowed patients to return home following an illness, injury, or surgery quicker than ever. Technology has also improved many ways healthcare providers work. These include a broad spectrum of activities, such as the ability to access a schedule, make changes from a mobile device, ensure appropriate supplies are where they need to be and determine when they are needed in order to provide the best possible patient care.
However, from a nurses’ perspective, there has been both a variety of successes and failures using technology in healthcare. Traditionally, everything from documenting patient care, to creating staff schedules, to ordering supplies was done on paper. On the other hand, some hospitals take a much more digitized approach, where every task performed seems to require the assistance of a computer and everything feels much faster paced.
At first glance, the hospitals that adopt all kinds of technology seem to make many improvements in patient care. Overall, it seems that patients have their needs tended to much quicker as a result of the technology solutions. For example, rather than someone tracking down a patient’s nurse when the patient needed assistance, the nurses could easily be reached by a phone that was always clipped to their waistband. The electronic medical record would automatically alert the caregivers if a medication was due, or if the patient had abnormal lab results or vital signs. The daunting task of filling out supply checklists so any supplies that were recently re-ordered had disappeared were no longer a time waster and the changes were amazing.
It still seems magical that Spotify creates a personalized music track for my life. Similarly, I now get personalized suggestions of what books to read, what recipes to cook, and even where to travel. This is the way we’re living our lives except for healthcare. It represents almost 20 percent of the U.S. economy and has a huge impact on my life, but I don’t have the ability to personalize my healthcare experience, personalize my medical treatments, or personalize how I’m treated as I move through the system.
What’s the missing piece? Data. We need to break data out of silos, exchange it, share it, leverage it, use it — all types of data — claims, clinical, new, and old. We can’t build personalized health without piecing together each patient’s individual experience to tell the full story. We cannot leverage the positive power of technology, including machine learning and AI, without data. Unlocking this information is difficult. But it’s critical work. And we need to democratize access to data, not treat it like a competitive asset, to bring the power of personalized medicine to every clinician and patient.
Data signals help patients personalize their choices
A nurse friend of mine has stage four breast cancer. Her clinicians gave her a treatment plan. But she took a close look at her health, her data, and the evidence and determined that in her particular case there was no evidence that the treatment options would extend her life, and they would probably cause her a lot of pain and suffering in the form of adverse effects. She decided not to get treatment and has lived a quite incredible life since then. Her doctors were surprised. But to her, it was simple — she didn’t want treatment because there was no evidence that it would work for her.
Data signals help care teams see the hidden patterns
We work with a care manager who follows up with patients after they have been in the hospital to help them get the care they need. Recently, she noticed a patient was getting treated at multiple emergency departments for falls. No one had noticed the pattern. But the care manager had access to the patient’s community health record from Manifest MedEx (MX) and could see the trend: The patient needed a walker. It did not take a huge amount of information or technology to deliver dramatically more effective and personalized care. It took data and someone to notice.
That’s the care we all want. We want healthcare that’s responsive to our needs, to our preferences, and to the simple things that make a difference.
You can’t personalize patient care without data
Exciting technology is in the pipeline to make the vision of personalized medicine a reality, but we don’t have a reliable health data infrastructure in place to power this future. It’s like saying you’re going to create self-driving cars, but there’s no GPS network.
Ten years ago, most data in healthcare was trapped on paper. Now, most — but not all — of it is digital. It’s huge that in just a decade we’ve been able to transition from paper to electronic data. And we are also getting better at sharing it.
But if we don’t have platforms to integrate it, match it to each patient, and identify signal, the data is just more noise for overburdened clinicians. If we want a future of personalized health, we’re going to have to make meaning from data. And this meaning needs to be available to everyone treating a patient.
By George Mathew, MD, chief medical officer, North America, DXC Technology.
George Matthew
Patients, like all consumers, are more digitally aware and connected than ever before, as they continue to embrace the latest mobile devices and wearables. These devices, as well as the increasing availability of information on health management, have made patients more engaged participants in managing their own health and wellness.
As a result, they demand timely access to their own health information and expect care services that are personalized and convenient. They also want to use consumer-friendly digital tools to engage with their clinical records, lab results, medications and treatment plans.
However, many health organizations are still evolving their approach to meet this challenge. Existing systems of record in healthcare are often siloed, making it difficult to share actionable patient information across the continuum to accelerate service delivery and improve outcomes. The solution lies in implementing next-generation digital health platforms to integrate sources of historical clinical and wellness data to derive insights that drive more engaging patient experiences, better outcomes and lower costs.
Bridging the Information Gap
Integrating data sources across healthcare segments and aggregating them into a single digital-patient record, empowers patients and providers to make better healthcare choices and improve quality of care.
Rather than searching and clicking across multiple systems, an integrated digital patient-care platform creates a “single source of truth” to give patients and their providers quick and easy access to real-time, context-specific information for timely decisions. Benefits include the following:
Providers can optimize clinical operations, with results that include streamlined processes, reduced patient admissions, shorter hospital stays and, ultimately, improved quality of care for patients.
Patients may obtain a full view of their complete health journey and access relevant education and medication information — instead of having to wait for follow-up visits to see and discuss their results.
Patient engagement can also be improved through secure patient messaging capability, the ability for providers to receive patient experience feedback, and deployment of intelligent virtual assistants across a range of mobile devices to create a connected healthcare experience.
Additionally, when healthcare staff have access to the most up-to-date data, they can ensure the right materials are in the right place, reducing material waste and minimizing patient wait times. Furthermore, integrating clinical and wellness systems can help providers efficiently collect population health data to maximize health outcomes through early interventions.