The world of healthcare is changing and those changes impact how we deliver care, our approach to engaging patients and the relationships between stakeholders across the healthcare value chain. Each day, we witness advances in genomics, imaging and pharmacology, and learn about the use of artificial intelligence (AI) to drive these advances. Indeed, healthcare is in the midst of a major revolution and AI seems to be at the very core of this transformation. How much of the AI story is hype and how much is real?
Innovaccer Inc., a San Francisco-based healthcare data activation company, is hosting a breakthrough AI webinar on June 20 with guest speakers Dr. Peter Lee, corporate vice president, Microsoft Healthcare, and Stephen K. Klasko MD, MBA, president and CEO, Thomas Jefferson University and Jefferson Health, who will be discussing the new healthcare domains of AI, and it’s “never imagined” impact. They will be joined by webinar moderator, David Nace MD, chief medical officer at Innovaccer.
The use of AI in healthcare has lagged behind other industries, in large part because of the lack of comprehensive, pristine data. The webinar, titled “Beyond Interoperability: Data Activation and Artificial Intelligence for Healthcare,” will focus on the recent AI hype, tease fact from fiction, and explain how advances in data activation can solve the accuracy and interoperability problems in the space.
Dr. Lee has extensive experience in managing the process of going from basic research to commercial impact. Past illustrative examples include the deep neural networks for simultaneous language translation in Skype, next-generation IoT technologies, and innovative silicon and post-silicon computer architectures for Microsoft’s cloud. He also has a history of advancing more “out of the box” technical efforts, such as experimental under-sea data centers, augmented-reality experiences for HoloLens and VR devices, digital storage in DNA, and social chatbots such as XiaoIce and Tay.
Lee is a member of the board of directors for the Allen Institute for Artificial Intelligence and the Kaiser Permanente School of Medicine. He served on President’s Commission on Enhancing National Cybersecurity. And, previously, as an office director at DARPA, he led efforts that created operational capabilities in advanced machine learning, crowdsourcing, and big-data analytics, such as the DARPA Network Challenge and Nexus 7.
Under Dr. Klasko’s leadership, Jefferson Health has grown from three hospitals in 2015 to 14 hospitals today. His 2017 merger of Thomas Jefferson University with Philadelphia University created a pre-eminent professional university that includes top-20 programs in fashion, design and health professions, coupled with the first design-thinking curriculum in a medical school, conducting the nation’s leading research on empathy, an essential component of medicinal practice that is often overlooked in the academic setting. As a disruptive leader in the academic ecosystem, Dr. Klasko brings a valuable point of view to the Innovaccer Strategic Advisory Council.
Few healthcare leaders doubt that insights made available through precision medicine and genomics have the potential to vastly improve care and outcomes.
But the industry struggles to overcome numerous barriers that, at first glance, seem to obstruct providers’ ability to fully leverage precision medicine. There is no question that obstacles exist, but a well-considered strategy can help providers move quickly down a forward path.
Let us consider the six primary obstacles to leveraging precision medicine to its fullest:
Provider education and expertise. Precision medicine, as an influencer at the point of care, is a nascent discipline. Few physicians practicing today were thoroughly educated in genomics (the depth of training is increasing, however, according to a 2017 article in the Association of American Medical Colleges News). Physicians find themselves in a position of educating themselves quickly, especially as the FDA approves more targeted immunotherapies and treatments. In addition, because of the rise of direct-to-consumer tests, patients themselves are demanding doctors factor this information into their clinical decision making.
Slow-to-change standards of care. Without a doubt, delivery of healthcare must be evidence-based. Genomic science has introduced so many advances in such a short period of time, however, that many physicians remain bound by approaches rapidly becoming outdated. The industry must find ways to deliver new findings into the clinical workflow reliably and quickly, so providers can utilize the best approach in each patient encounter.
Limited time to process new data. Physicians are already presented with more data than they can effectively manage. Genomics represents an entirely new and voluminous data set. To deliver any value, this information must be rendered useful and readily available within the EHR. Access must be smooth and seamless so physicians are not forced to leave their workflow to hunt for relevant insights.
Foreign nomenclature. Currently, genomic results are returned in PDFs (not as discrete data), rendered in vocabulary common to genomic researchers and scientists. It must be “translated” into meaningful clinical nomenclature and then integrated into the current workflow to be fully useable.
Regulatory and liability concerns. Genomic results do not represent a snapshot in time the way phenotypical information might. A patient’s genetic variant could impact care decisions well into the future as the individual’s condition changes and genomic science advances. How does a provider store and manage genomic data, making sure that its very existence does not create liability issues in the years ahead?
Lack of or sluggish reimbursement. Payer policies and guidelines lag behind discoveries related to precision medicine. What reimbursement exists varies greatly from payer to payer and is founded on disparate understandings of medical necessity. While payment is becoming more common, physicians nevertheless must consider the financial impact of ordering a genomic test – and what they will do if the results indicate that an expensive or uncommon treatment is the best choice for a particular patient.
By Chris Talbot, senior vice president of marketing and business development, Ascom.
Chris Talbot
More than 4,900 U.S. hospitals participate in the Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS), including 3,529 that received star ratings in the most recent quarterly update. These ratings reflect an effort by the Centers for Medicare & Medicaid Services (CMS) to help consumers make informed choices about their care, putting more decision-making and purchasing power in their hands.
Because star ratings are expected to play an increasing role in helping consumers choose hospitals, it is important to understand these metrics and what hospitals can do to improve their performance.
Toward that end, Ascom created a comprehensive, time series database of hospital HCAHPS performance.
Changes to hospital Star Ratings over time
Leveraging our database, we conducted a year-over-year analysis of star ratings for all participating hospitals, providing insights into how star ratings change over time as well as clues to what it may take to improve performance.
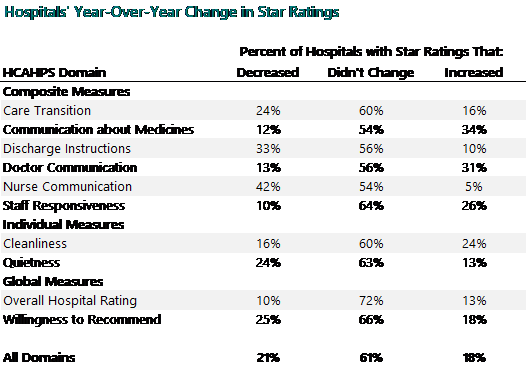
As shown in the table below, our analysis revealed that star ratings tend to be sticky. In our year-over- year comparison across all hospitals, 61 percent of ratings remained unchanged. Overall, only 18 percent of ratings improved over a 12-month period, while 21 percent declined.
Why Star Ratings are slow to change
There are two main reasons that hospitals’ star ratings tended not to change over a 12-month period.
Because the quarterly HCAHPS results include four quarters’ worth of survey data, it can take a while for improvements to show up in the ratings. Even if a hospital achieves significant improvements in its most recent quarter, that quarter’s results are combined with the previous three quarters’ poorer results when they are reported by CMS.
There is also the difficulty of the task at hand. It’s not just a matter of providing excellent patient care – which is difficult enough; it’s also a matter of providing this level of care at the highest level of consistency.
Consistency is the key to improvement
Consistency is important at two levels. The first is across the HCAHPS domains. While HCAHPS monitors several different individual domains such as care transition, cleanliness, etc., they all add up to a total experience across each individual patient’s journey.
Our correlation analysis between all the linear mean scores for all HCAHPS domains found that if a patient’s satisfaction with one domain was high, then satisfaction with all domains tended to be high and vice versa. This in turn drove overall satisfaction with the hospital, and patient likelihood to recommend the hospital to others.
Any patient matching improvement strategy must look beyond technology and emphasize the people and processes that play a critical, yet often overlooked, role in ensuring data integrity. That was the message Just Associates, Inc., shared with the Centers for Medicare and Medicaid Services (CMS) and the Office of the National Coordinator for Health IT (ONC) in response to requests for information on patient matching in conjunction with proposed rules to advance interoperability.
In its letter to the ONC, Just Associates noted that while it supports the focus on interoperability and usability and agrees with the importance of accurate patient matching, it does not believe that the concept of a “technology alone” solution is realistic. Any improvement strategy must also include data standardization and promote a more consistent, comprehensive collection of patient data at all entry points.
“Every technology has its flaws when it comes to patient matching and the importance of training staff, developing and maintaining comprehensive data governance policies, ensuring executive support for data governance and vigilant efforts on measuring and reporting data quality are critical. We cannot ignore the ‘people and process’ aspects to obtaining high levels data quality,” the letter stated.
Just Associates also provided feedback to the ONC on the importance of consistently defined and used format constraints and identified key issues that must be addressed to accurately measure algorithm performance. The suggestion was also made to align with the Children’s Hospital Association’s temporary demographic conventions for newborns to address the unique challenges with pediatric matching.
In its letter to CMS, Just Associates concurred with the suggestion that more standardized data elements be used across all appropriate programs to immediately enhance matching rates, noting that “data collection standards and their consistent application by health plans, providers and exchange organizations are critical for matching accuracy.
“Equally important,” the letter continued, “is the development of data definitions for these elements to ensure common understanding of exactly what data is being collected and in what format.”
Other advice offered by Just Associates in response to CMS suggestions included avoiding mandating the use of specific matching algorithms, data sources or software solutions, a move that would likely be premature and overly prescriptive. The firm also stated its support for implementation of a CMS-wide identifier, noting its potential to enhance accuracy and assist in duplicate record reconciliation verification processes.
By Dr. Chris Hobson, chief medical officer, Orion Health.
Dr. Chris Hobson
Health information exchanges (HIE) help care teams provide more informed patient care by supplying a complete longitudinal healthcare history of the patient to healthcare professionals, as well as enabling high quality reporting and analytics on the data. The goal of an HIE is to accurately store all relevant patient information from as many sources as possible, including medical history, medication history, past treatments and detailed personal information. A comprehensive reporting system allows for health delivery that is more responsive and tailored to each patient, and subsequently, the broader population.
Today the transition to value-based funding models seeks to lower costs and improve patient care and outcomes in order to lead to the better management of entire populations. Population health management (PHM) involves changing the behavior of engaged consumers to lead healthier lives and encouraging physicians to focus on providing the best possible quality of patient care at the lowest possible price. This requires providers to collaboratively address whole populations and orchestrate healthcare provision at large scale. Below are several challenges organizations must overcome before closing in on the goal of PHM.
Payer-provider collaboration and targeted incentives
Payers and providers must work together and, in particular, must find ways to effectively share their different types of data. Collaboration is needed to achieve shared goals such as understanding and improving the health of a population and enhancing the patient experience, all while constraining costs.
A key issue between payers and providers is agreement on the quality measures that will be incentivized. PHM places an unfair, high burden on providers if required quality measures vary widely across payers or if the measure does not clearly reflect a meaningful quality of care indicator. In the latter situation, a provider’s time and effort are used for inefficient purposes adding to a physician’s frustration with the healthcare system. Conversely, payers have additional data that can often help providers significantly with their population health management needs.
Care coordination
Fragmentation of care poses a challenge for health systems globally, and there is research to suggest that this problem is more persistent in the U.S. than its international peer countries. Studies have highlighted the major consequences of a poorly coordinated health system, including delays in care, incorrect care, and unnecessary complications, tests and procedures. Frequently, poor communication, difficulty sharing care plans and challenges coordinating actions by multiple caregivers across organizations results in confusion, delays in care and even incorrect care actions, putting the patient’s health on the line. A health system that is not well coordinated cannot deliver high quality care at lower costs.
Physician involvement in preventive care and the social determinants of health
For physicians, finding ways to move care from the acute setting toward health promotion, disease prevention and addressing the social determinants of health is quite difficult and not something they are necessarily empowered to do today. Currently, the majority of physicians do not have the tools to solve major intractable social issues such as poverty, so involving physicians and patients in the strategic design of a social determinants of health program is an essential step toward resolution of these types of concerns.
Cyber terrorists have made their way into hospitals, and they are targeting ultrasound machines specifically. It appears there is a black market for this content, and people are paying good money for it.
A big reason for this is health machines are running on ancient software. The cyber terrorists use encryption to access the data from ultrasound machines. Since many health sector employees are not knowledgeable about cybersecurity, it’s an easy target and this is why they are getting a beat from cyber-terrorist.
The issue
Medical equipment today uses ancient hardware and software. Some of these machines are still running on Windows 2000. Microsoft had long cut off their support for Windows 2000, Windows 95 and Windows XP.
Thanks to the outdated software, cyber terrorists can easily get hold of the patient’s sensitive information. This can cost both the hospital and patient a fortune in ransom.
Anyone who accesses a hospital’s network can easily access all the records. Worse, they can connect to ultrasound imaging devices that are vulnerable to attacks because they use ancient software. Once you breach the network, getting access to details images and other details become very easy. It’s very scary for patients and hospitals that ultrasound machines are vulnerable to hacking.
The wake-up call
There was an attack in 2017, called the WannaCry virus. This virus targeted computers running on old Microsoft Windows systems. It could cause millions of dollars of loss.
These attacks have stolen $92 million. The underlining learning lesson was that you are a hacking target when using an ancient OS that doesn’t have updates and patches regularly.
How to solve this?
Hospitals are responsible for protecting the critical information of their patients. So, it will be a lot better if they start using encryption on their network and files. They can employ someone who can encrypt all of their stuff or use an application to do so.
Healthcare data hacking has started occurring pretty often nowadays and most people are not even aware that their data has been stolen. Healthcare organizations are not built in a way they can identify illegal records; hence, they are unable to eliminate them.
The main problem is that people are not aware of healthcare data breach until they are sick and need treatment, which makes it the worst time to deal with problems like this. Breaching of healthcare data leads to losing insurance coverage, mixed up records, wrong diagnosis, medical harm, etc.
Thus, how do you prevent this from happening? Here are here to share some tips that will help you avoid healthcare data hacking.
5 Tips to avoid healthcare data hacking
Lexington Law. Healthcare data theft, along with Identity theft, has become a huge problem in today’s world. In order to stay protected from these things, hiring services like Lexington law can be extremely helpful.
They provide things like free credit report evaluation and attractive discounts for couples, families and active military personnel along with protecting your health care data and identity. You can go over to websites, like Crediful, to read a review about Lexington law before buying.
Do a risk assessment test. In 2003, a rule was passed by HIPAA which stated that healthcare organizations were required to take a risk assessment test. However, there was no penalty if not done, so most organizations did not do it.
Then the HITECH Act passed and it changed the law by making security risk analysis mandatory. Performing security analysis helps in identifying vulnerabilities in the security systems and identifying threats.
Always keep software up to date. Most people neglect software updates as they are busy and do not like the idea of taking the computer system offline for updates, but this is a terrible thing to do, and it puts your data on a huge risk.
The latest version of the software is mainly released to reduce any security risks, and not updating them keeps your devices vulnerable to threats and attacks. You will miss any security patch that comes with the latest updates. Criminals use this to their advantage to steal data from outdated devices. Thus, make sure you always keep all software updated.
The healthcare industry has a dupe problem. Today, on average, providers are seeing almost one in five of their patients’ records contain duplicates (meaning that two or more records are in existence with a variation of a patient’s name), according to a report by Black Book. This represents a significant threat as it can potentially lead to inaccurate billing and compromised patient safety. For years, providers have invested heavily in technology and systems designed to improve operational efficiency (while also mitigating the number of duplicate records) yet the problem persists.
According to the same report by Black Book, duplicate medical records cost an average hospital $1.5 million annually – and those are 2017 numbers, so today’s impact is even higher. The average cost of repeated medical care due to inaccurate patient identification with a duplicate record is roughly $1,950 per inpatient stay and more than $800 per emergency department visit. Likewise, A study from Boston Children’s Hospital estimates that one in three patients received duplicate tests because of duplicate health records.
It seems like a simple enough problem to solve, so why is it still so pervasive? As with so many issues in the complex world of healthcare, there is no single cause to the problem. Most commonly, the origin of duplicate records can be traced to a rushed patient intake experience — one that often leads to human error like typos; misunderstanding words or phrases due to language barriers and accents; or harried friends and relatives scrambling to remember information in an effort to assist loved ones in medical distress.
Additionally, patient name changes, due to common instances like marriage and divorce, aren’t often reported to healthcare providers in the expedient manner that they are with other agencies. Combine these factors with infrequent patient visits and the data quickly becomes inaccurate, resulting in duplicate records.
Pressure to act
As if these factors aren’t enough, the Office of the National Coordinator for Health Information Technology (ONC) has published industry-wide patient matching error goals of 2 percent by 2017, 0.5 percent by 2020 and 0.01 percent by 2024. For the many organizations that have yet to achieve the stated 2017 goal, the far more stringent 2020 standard presents a daunting challenge.
Although there is no mandate or enforcement mechanism attached to these goals at present, it’s not hard to envision the government taking a more aggressive approach in the absence of demonstrable industry-wide progress. The hard truth is that many organizations do not currently have plans in place that would even make it possible to demonstrate progress. Many continue to leverage the same processes and legacy technology that have been in place for years and find themselves no closer to meeting the ONC’s deadlines.



 Cyber terrorists have made their way into hospitals, and they are targeting ultrasound machines specifically. It appears there is a black market for this content, and people are paying good money for it.
Cyber terrorists have made their way into hospitals, and they are targeting ultrasound machines specifically. It appears there is a black market for this content, and people are paying good money for it. Healthcare data hacking has started occurring pretty often nowadays and most people are not even aware that their data has been stolen. Healthcare organizations are not built in a way they can identify illegal records; hence, they are unable to eliminate them.
Healthcare data hacking has started occurring pretty often nowadays and most people are not even aware that their data has been stolen. Healthcare organizations are not built in a way they can identify illegal records; hence, they are unable to eliminate them.