Over the last few decades, we have seen exponential growth in technology. Hardware and software permeate the world around us. The world has become a smaller place with distances presenting less of an obstacle. Businesses manage employees across the globe with remote collaboration software. We see advanced satellites going into space, mapping the unknown. We know much more about geology thanks to sophisticated equipment.
Technology is evolving very fast, and so is the health sector. However, the impact of technology has been most profound in the field of medicine. This blog discusses how.
Technology in the health sector
Technology has played an important role in improving healthcare. We have advanced treatments and procedures that seem commonplace today. The improvement itself has been constant. You can see it from the invention of X-rays to precise surgical procedures. These advancements have made it possible for humans to live healthier lives. They have resulted in a longer average life expectancy. As we go into the 21st Century, there is no reason to suppose that technology is slowing this process down. The most recent example is medical science developing a promising AIDS treatment. Technology and science help cure diseases and improve the quality of our lives even more. Here are only four ways in which technology is improving the health sector:
Gene sequencing
Wearable medical devices
Remote medical monitoring
Digital medical records
Let’s take a closer look at how technology impacts these specific areas in the health sector.
Gene sequencing
Human genomics has earned a reputation as the future of medical science. What gene sequencing refers to is sequencing and analyzing a person’s genome. This information also goes to the person. Sequencing the human genome is one of humanity’s biggest achievements. Especially in the last four decades. The human genome is like an instruction manual for the human body. It may help people detect and avert hereditary diseases and live a better life.
Recent research was published by the Washington Post about malware that was created to disrupt medical imaging equipment and networks. This is yet another wake-up call for the healthcare industry that been underinvesting in security for the last decade. Quite simply, there is a misconception that hospitals’ internal networks are a safe harbor from external cyberattacks. This is despite the fact that the real-world data has repeatedly shown that healthcare is one of the top industries under attack for the last five years. While previous attacks mainly focused on stealing personal health information, this research demonstrates how serious or even deadly an attack to healthcare can be.
There are a few reasons why cyberattacks in healthcare today can have devastating consequences.
Medical device vulnerabilities
Many medical devices inside hospitals are running decade old operating systems and applications that have many well-known vulnerabilities. In fact, it may be a surprise to many that the vast majority of imaging systems run on Windows OS. Further, recent Zingbox research shows that today, 1 out of 4 imaging systems run on OSes that are no longer supported. By next year, 85% of imaging systems are expected to run on End-of-Lifed OSes as Microsoft terminates support for some of their popular Windows OSes.
To make matters worse, most medical device manufacturers lack strong in-house cybersecurity expertise. While their expertise lies in device reliability and accuracy, which continue to be top requirements for connected medical devices, the lack of cybersecurity expertise puts the device reliability and accuracy into question. The lack of cyber-specific expertise also limits manufacturers’ ability to “bake in” cybersecurity measures on the device.
One might think that patches and upgrades are the answer. Unfortunately, no. FDA certification and other requirements pose significant hurdles for manufacturers to apply patches or upgrades to devices already deployed at hospitals.
Tools designed for IoT
Many hospitals lack the tools to monitor life-critical devices with 100% assurance of uninterrupted service and care. Such tools must be completely transparent to the device and in no way interfere or hamper its operation. Yet, organizations continue to rely on traditional IT security solutions for IoT. Such network security tools like firewalls and antiviruses result in security gaps that hackers can easily exploit.
Vulnerabilities that stem from inadequate IoT security tools:
Most network security solutions often cannot discern a PC from a CT scanner, whereas such a distinction is critical for cybersecurity.
CT scanner’s communication is almost never encrypted, device access doesn’t require basic authentication, and given the mobility of typical CT scanners, the devices can be connected to any internal network, according to Zingbox’s research findings.
Connecting a device to any network breaks the basic micro-segmentation policies IT teams have been encouraged to deploy for cybersecurity.
Today, the Trump Administration proposed changes to further the agency’s priority to transform the healthcare delivery system through competition and innovation while providing patients with better value and results. The proposed rule would update Medicare payment policies for hospitals under the Inpatient Prospective Payment System (IPPS) and the Long-Term Care Hospital (LTCH) Prospective Payment System (PPS) for fiscal year 2020 and advances two key CMS priorities, “Rethinking Rural Health” and “Unleashing Innovation,” by proposing historic changes to the way Medicare pays hospitals.
“One in five Americans are living in rural areas and the hospitals that serve them are the backbone of our nation’s healthcare system,” said CMS Administrator Seema Verma. “Rural Americans face many obstacles as the result of our fragmented healthcare system, including living in communities with disproportionally higher poverty rates, more chronic conditions, and more uninsured or under insured individuals. The Trump Administration is committed to addressing inequities in healthcare, which is why we are proposing historic Medicare payment changes that will help bring stability to rural hospitals and improve patients’ access to quality healthcare.”
The inpatient hospital wage index specifies how inpatient payment rates are adjusted to account for local differences in wages that hospitals face in their respective labor markets. It is intended to measure differences in hospital wage rates across geographic regions and is updated annually based on wage data reported by hospitals. Hospitals located in areas with wages less than the national average receive a lower Medicare payment rate than hospitals located in areas with wages higher than the national average. For example, a hospital in a rural community could receive a Medicare payment of about $4,000 for treating a beneficiary admitted for pneumonia while a hospital in a high wage area (like many urban communities) could receive a Medicare payment of nearly $6,000 for the same case, due to differences in their wage index.
In last year’s proposed rule, CMS invited comments on changes to the Medicare inpatient hospital wage index. Many responses reflected a common concern that the current wage index system makes the disparities between high and low wage index hospitals worse. High wage index hospitals, by virtue of higher Medicare payments, can afford to pay their staff more, allowing the hospitals to continue operating as high wage index hospitals. Conversely, low wage index hospitals often cannot afford to pay wages that would allow them to climb to a higher wage index. Over time, this creates a downward spiral that increases the disparity in payments between high wage index hospitals and low wage index hospitals, and payment for rural hospitals and other low wage index hospitals declines.
To address these disparities, CMS is proposing to increase the wage index of low wage index hospitals. This change would ensure that people living in rural areas have access to high quality, affordable healthcare. CMS is considering several ways to implement this change, and the agency looks forward to comments on the different approaches.
The Trump Administration is also announcing proposals that would ensure Medicare beneficiaries have access to a world-class healthcare system by unleashing innovation in medical technology and removing potential barriers to innovation and competition in order to expedite access to novel medical technology.
“Transformative technologies are coming to the private market, but Medicare’s antiquated payment systems have not contemplated these technologies,” said Verma. “I am particularly concerned about cases that have been reported to the agency in which Medicare’s inadequate payment has led hospitals to curtail access to needed therapies. We must continually update our policies in response to the rapid pace of advancement in medical science.”
U.S. Department of Health and Human Services (HHS) Secretary Alex Azar and Centers for Medicare & Medicaid Services (CMS) Administrator Seema Verma announce the CMS Primary Cares Initiative, a new set of payment models that will transform primary care to deliver better value for patients throughout the healthcare system. The CMS Primary Cares Initiative will aim to reduce administrative burdens and empower primary care providers to spend more time caring for patients while reducing overall healthcare costs, HHS said in a statement.
Alex Azar
“For years, policymakers have talked about building an American healthcare system that focuses on primary care, pays for value, and places the patient at the center. These new models represent the biggest step ever taken toward that vision,” said HHS Secretary Alex Azar. “Building on the experience of previous models and ideas of past administrations, these models will test out paying for health and outcomes rather than procedures on a much larger scale than ever before. These models can serve as an inflection point for value-based transformation of our healthcare system, and American patients and providers will be the first ones to benefit.”
Empirical evidence shows that strengthening primary care is associated with higher quality, better outcomes, and lower costs within and across major population subgroups. Despite this evidence, primary care spending accounts for a small portion of total cost of care, and is even lower for patients with complex, chronic conditions, HHS said.
CMS’s experience with innovative models, programs and demonstrations to date have shown that when incentives for primary care clinicians are aligned to reward the provision of high-value care, the quality and cost effectiveness of patient care improves, the organization cited.
Seema Verma
“As we seek to unleash innovation in our health care system, we recognize that the road to value must have as many lanes as possible,” said CMS Administrator Seema Verma. “Our Primary Cares Initiative is designed to give clinicians different options that advance our goal to deliver better care at a lower cost while allowing clinicians to focus on what they do best: treating patients.”
Administered through the CMS Innovation Center, the CMS Primary Cares Initiative will provide primary care practices and other providers with five new payment model options under two paths:
Primary Care First and Direct Contracting.
The five payment model options are:
Primary Care First (PCF)
Primary Care First – High Need Populations
Direct Contracting – Global
Direct Contracting – Professional
Direct Contracting – Geographic
The Primary Care First (PCF) payment model options will test whether financial risk and performance based payments that reward primary care practitioners and other clinicians for easily understood, actionable outcomes will reduce total Medicare expenditures, preserve or enhance quality of care, and improve patient health outcomes. PCF will provide payment to practices through a simplified total monthly payment that allows clinicians to focus on caring for patients rather than their revenue cycle. PCF also includes a payment model option that provides higher payments to practices that specialize in care for high need patients, including those with complex, chronic needs and seriously ill populations (SIP).
Both models under PCF incentivize providers to reduce hospital utilization and total cost of care by potentially significantly rewarding them through performance-based payment adjustments based on their performance. These models seek to improve quality of care, specifically patients’ experiences of care and key outcome-based clinical quality measures, which may include controlling high blood pressure, managing diabetes mellitus and screening for colorectal cancer. PCF will be tested for five years and is scheduled to begin in January 2020. A second application round is also planned for participants starting in January 2021.
By Chris Jaeger, head of ACO and health system strategy, AristaMD.
Rural hospitals are facing severe challenges in maintaining operating margin, with uncompensated care being a major factor. Telehealth eConsult platform use in local primary care settings to improve “right time, right place, right provider care” have been shown to decrease the number of patients receiving avoidable and unnecessary care within the hospital setting, thus supporting hospital’s ability to mitigate uncompensated care.
Uncompensated care is an overall measure of hospital care provided for which payment was not received from the patient or payer group. It equates to the sum of a hospital’s bad debt — the financial assistance it provides. Financial assistance includes care for which hospitals never expected to be reimbursed and care provided at a reduced cost for those in need. A hospital incurs bad debt when it cannot obtain re-imbursement for care provided; this happens when patients are unable to pay their bills, but do not apply for financial assistance, or are unwilling to pay their bills.
Hospitals, both nonprofit and for-profit, provide uncompensated care for individuals who are uninsured and under insured.
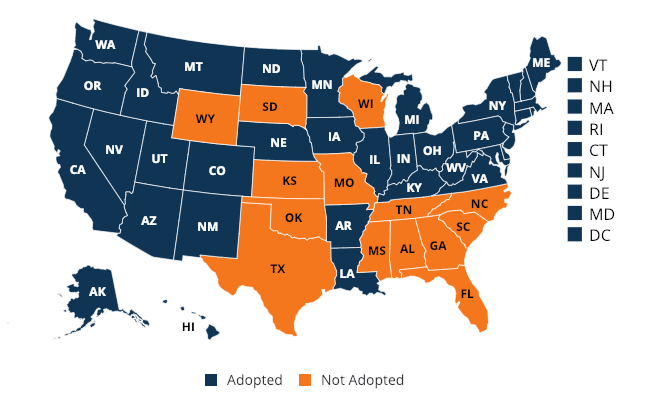
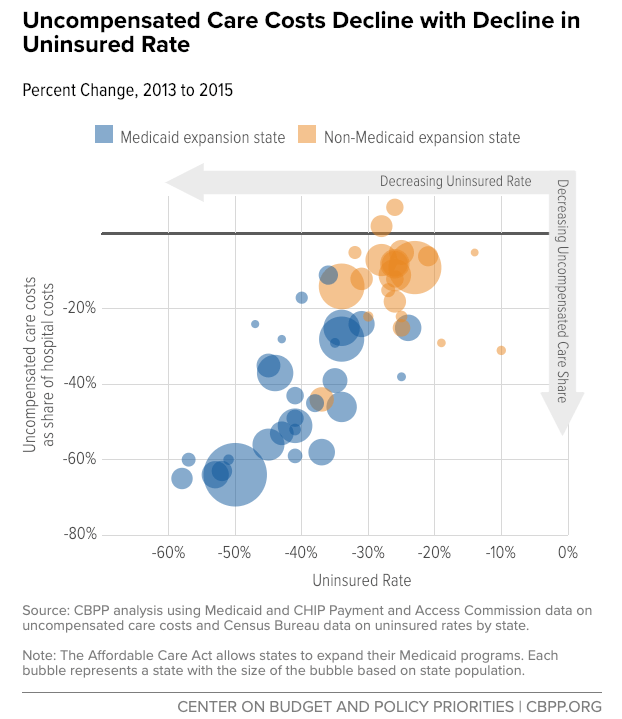
Though there has been a noted decline in uncompensated care since the 2014 passage of the Affordable Care Act and Medicaid expansion, this has not carried over to states not part of the expansion. States that expanded Medicaid to low-income adults under the ACA recognized a 47 percent decrease in uncompensated care costs, on average, compared to an 11 percent decrease in states that did not expand Medicaid.
(Coverage map as of Feb 2019)
Uncompensated care and dropping revenue margins are causing hospitals, especially in rural areas, to close. “While Medicaid expansion has improved all hospitals’ operating margins and total margins, the effect was particularly pronounced in rural areas,” noted a report from the Center on Budget and Policy Priorities. A recent study by the North Carolina Rural Health Research Program (NC-RHRP) at the University of North Carolina Cecil G. Sheps Center for Health Services Research (UNC-CH) showed that since 2010, 89 rural hospitals in 26 states have closed.
Much of this uncompensated care could be prevented through primary care intervention. A report, released by Premier, found that six common chronic conditions accounted for 60 percent of 24 million Emergency Department (ED) visits in 2017; out of that 60 percent, approximately one third of the visits (4.3 million) were likely preventable and could be treated in a less expensive outpatient setting.
One of the biggest trends in healthcare has a distinctly technical focus: clinical mobility, the use of mobile devices like smartphones, tablets, laptops, and mobile printers by physicians and nurses at the point of care. According to the U.S Department of Health and Human Services, the average physician currently spends 15 hours per week on reporting measures, cumulatively costing a staggering $15.4 billion annually. Added mobility measures will be a huge relief to these healthcare heroes, who can then spend more time with patients.
The requirements for devices utilized by medical professionals are exacting and stringent because our health depends on them. Likewise, many devices must comply with the sweeping Health Insurance Portability and Accountability Act (HIPAA) regulations, along with numerous other government certifications. While there is a plethora of mobile healthcare devices on the market, a select few are worth calling out for the progress in their performance and usage. Here are three essential tools for modern practices.
Location technologies
No hospital or clinic can survive without positive patient identification (PPID) wristbands, which track patients from admission to discharge using printed labels and help improve throughput and security. Staff members scan bar codes on the bracelets to access medical history, medication lists, or allergies and then send data directly to labs or pharmacies through hospital databases. Workers can also use PPID to generate labels for everything from charts and bills to specimen containers, so important medical documents and paraphernalia stay secure.
Assisted living facilities and nursing homes that give patients more freedom benefit from PPID as well, because the technology is excellent at helping maintain the safety of residents. In many cases, family members can also access this information, and so have peace of mind.
Personal care technologies
Chatbots have revolutionized many areas of modern life, and medicine is no exception. The artificially intelligent apps handle basic but time-consuming tasks, ensuring patients take prescriptions and comply with orders. These tools will save the healthcare industry billions of dollars, so many tech companies want to get in on the action, such as by using text and voice apps to answer patient questions with natural language processing, helping medical professionals stay mobile and focused on their work.
By David A. Watson, chief executive officer of Akiri, and former CTO, Kaiser Permanente.
David Watson
The American Medical Association (AMA) identifies one of the biggest challenges in healthcare today as the secure sharing and use of trusted health data in real time across the complex U.S. healthcare ecosystem. To hijack a Winston Churchill quote — data liquidity is a riddle wrapped in a mystery inside an enigma. The key to solving this puzzle is not more technology; we’ve had good integration technology for 30 years. What we need is a fundamentally different approach that addresses the adoption issues that have so far prevented success.
Do we face challenges caused by the inability to accurately identify different fragments of patient data coming from different systems producing incompatible data that is exacerbated by incomplete or inadequate data standards? Absolutely. And they are being addressed – albeit slowly – by the technology community. The more intractable problem is adoption. That challenge can be boiled down to three overlapping issues which hinder productive health outcomes:
Trust – there is insufficient trust among the healthcare data trading partners (e.g., healthcare organizations fear that shared data could result in some sort of business disadvantage).
Economic Incentive – there is no direct economic incentive for those who possess the data (and bear the cost of creating/communicating it) to share it with those who need it (and who benefit from it).
Control – organizations that share their data want to have a sense of control regarding what is being shared with whom.
Achieving data liquidity in the sprawling systems that make up the U.S. healthcare economy requires a combination of rethinking the applied technology to make it easier and less expensive, while closing the adoption gap by giving the participants in data exchange solid business reasons to do so. Without addressing the economic issues and retaining a strong privacy compliance footprint, no amount of technology will overcome the market entropy noted above.
Today, the U.S. Department of Health and Human Services (HHS) announced it is extending the public comment period by 30 days for two proposed regulations aimed at promoting the interoperability of health information technology (health IT) and enabling patients to electronically access their health information. The new deadline for the submission of comments – June 3, 2019 – will allow additional time for the public to review the proposed regulations.
The extension of the public comment period coincides with a release by the HHS Office of the National Coordinator for Health Information Technology (ONC) of the second draft of the Trusted Exchange Framework and Common Agreement, along with a related Notice of Funding Opportunity. HHS also today released of a set of frequently asked questions (FAQs) from the Office for Civil Rights (OCR).
The FAQs address the Health Insurance Portability and Accountability Act (HIPAA) right of access as it relates to apps designated by individual patients and application programming interfaces (APIs) used by a healthcare provider’s electronic health record (EHR) system. The FAQs clarify that once protected health information has been shared with a third-party app, as directed by the individual, the HIPAA covered entity will not be liable under HIPAA for subsequent use or disclosure of electronic protected health information, provided the app developer is not itself a business associate of a covered entity or other business associate.
On February 11, 2019, HHS announced two proposed rules to support the seamless and secure access, exchange, and use of electronic health information (with Federal Register publication on March 4, 2019). The rules would increase choice and competition while fostering innovation that promotes patient electronic access to and control over their health information. Together the proposed rules address both technical and healthcare industry factors that create barriers to the interoperability of health information and limit a patient’s ability to access essential health information. Addressing those challenges will help to drive an interoperable health IT infrastructure across systems, enabling healthcare providers and patients to have access to health data when and where it is needed.
This extension responds to requests from a variety of stakeholders, including healthcare provider organizations and industry representatives. The Centers for Medicare & Medicaid Services (CMS) and ONC understand that both rules include a range of issues having major effects on healthcare. The extension of the public comment deadline will maximize the opportunity for meaningful input and further the overall objective to obtain public input on the proposed provisions to move the healthcare ecosystem in the direction of interoperability.
For more information on the Trusted Exchange Framework and Common Agreement and the Notice of Funding Opportunity, visit: https://www.healthit.gov/TEFCA


 “One in five Americans are living in rural areas and the hospitals that serve them are the backbone of our nation’s healthcare system,” said CMS Administrator Seema Verma. “Rural Americans face many obstacles as the result of our fragmented healthcare system, including living in communities with disproportionally higher poverty rates, more chronic conditions, and more uninsured or under insured individuals. The Trump Administration is committed to addressing inequities in healthcare, which is why we are proposing historic Medicare payment changes that will help bring stability to rural hospitals and improve patients’ access to quality healthcare.”
“One in five Americans are living in rural areas and the hospitals that serve them are the backbone of our nation’s healthcare system,” said CMS Administrator Seema Verma. “Rural Americans face many obstacles as the result of our fragmented healthcare system, including living in communities with disproportionally higher poverty rates, more chronic conditions, and more uninsured or under insured individuals. The Trump Administration is committed to addressing inequities in healthcare, which is why we are proposing historic Medicare payment changes that will help bring stability to rural hospitals and improve patients’ access to quality healthcare.”


 Today, the U.S. Department of Health and Human Services (HHS) announced it is extending the public comment period by 30 days for two proposed regulations aimed at promoting the interoperability of health information technology (health IT) and enabling patients to electronically access their health information. The new deadline for the submission of comments – June 3, 2019 – will allow additional time for the public to review the proposed regulations.
Today, the U.S. Department of Health and Human Services (HHS) announced it is extending the public comment period by 30 days for two proposed regulations aimed at promoting the interoperability of health information technology (health IT) and enabling patients to electronically access their health information. The new deadline for the submission of comments – June 3, 2019 – will allow additional time for the public to review the proposed regulations.