Anyone who is interested in signing up for Medicare has many decisions to make, including which type of insurance plan to go with to the type of physicians that they are on the plan. Those living in Florida for example can register a Florida LLC, same with other localities based on existing regulations. But one decision that is particularly important is between using Medicare Advantage plans or going with the more traditional approach to insurance, called Medicare Part A and Part B.
Medicare Part A and Part B
Many people are choosing to stay on their current health plan, called Medicare Part A. The benefits are similar to those of Medicare Part B, except that there is no co-payment required and there are no annual limits on how much you can spend. These plans are also known as Parts A and B. While some doctors agree with the advantages of this type of insurance, other physicians and hospitals are opposed to the use of these plans.
Medigap
Those who are choosing a different type of Medicare coverage are often opting for Medigap, which means that they have an additional deductible, which is why they pay more out-of-pocket. Most people think that if they have a large hospital bill, they will not be able to afford the Medigap premium, so they use Part A instead. However, those with medical conditions that require higher doses of medication, such as heart conditions, kidney diseases or cancers, may be able to qualify for Medigap as a supplement to the original Medicare plan.
Should you find yourself in an emergency situation where your airway constricts, or you lose consciousness, dialing 911 and communicating with an operator won’t lie within the realm of possibility.
If you currently live alone or have an immediate family member who lives alone, a choking incident or fainting spell can become terminal in the blink of an eye.
To ensure vulnerable and high-risk populations are safe from any slips, falls, and unexpected accidents, consider purchasing a panic-button device.
The sad reality is seniors can sustain life-altering injuries after slipping in the shower or tripping over untidied clutter. Because of limiting mobility restrictions, balance issues, and chronic ailments, seniors are vulnerable and are at risk of medical and other emergencies.
Given the nature of their health condition, a minor injury can render this high-risk demographic immobile and unable to contact emergency services. If these senior citizens live alone and fall out of arm’s reach from a telephone, shouting for help won’t be possible.
Fortunately, thanks to technological advancements, panic-button devices offered by companies like Lively Direct can enhance senior citizens’ quality of life. With panic buttons, help is just minutes away with a push of a button.
Are you curious to learn more about the benefits of using a panic-button device for seniors? Read on for more information on how these devices can radically transform your elderly loved one’s day-to-day life.
Key benefits of a panic button for the seniors
You’ve probably heard or read about panic buttons. Whether these panic-button commercials acted as background noise in your living spaces or piqued your interest, it’s time to pay closer attention to these state-of-the-art panic devices. If you’re currently struggling with mobility restrictions or worried about an elderly loved one toppling over, you’ll need to conduct the necessary research and read about the benefits these devices yield.
Immediate medical assistance
The thought of seniors living alone and struggling to request immediate medical assistance when they need it can strike fear into the hearts of any family member or loved one. When we think of emergencies that directly impact senior citizens, falling often comes to mind. And quite frankly, these incidents are worthy of concern. Let’s look at some statistics.
By Bill Flatley, senior service delivery manager, OST.
Bill Flatley
When the global pandemic hit the United States in March, droves of people who normally would have visited hospitals or clinics for routine care and appointments stayed home. Whether out of a fear of being contaminated or due to adhering to the stay at home mandates, sick visits to hospitals and doctor’s offices declined for many individuals who instead opted for telehealth appointments.
March and April saw a peak in the telehealth surge, with a slowdown period going into June and July as more states opened back up. Despite this slowdown, telehealth is here to stay with a higher utilization than any pre-COVID-19 times. Whether it’s hospitals or family practice clinics, many have discovered that there could be better care pathways or standard of care for various patients, that telehealth fits just fine.
Use cases will increase as digital health platforms become more robust and available. In order to aid in the efficacy of telehealth appointments, people now can take home commercial-grade devices to test and gather certain vital signs, making it available to their physician. For example, a patient can take home a kit that takes several different vitals and have it flow right back into a digital health platform, from there it can integrate directly into the electronic health record systems. The greater flexibility this allows will increase the amount of telehealth visits since patients can be anywhere and yet physicians will be able to provide better care through receiving more patient data.
Where telehealth loses steam
Telehealth loses steam when physicians find flaws and burdensome workflows. Part of third-party application development is making sure all of the components integrate into the electronic health record and keep the physician in the EHR while not forcing them to log into multiple, different systems. Through streamlined applications, physicians will feel less burdened and it will ultimately boost utilization.
Another challenge of implementing telehealth is putting the burden on physicians to set up the actual online interaction. To minimize this, it is important to build new workflows within digital health platforms and the electronic health record making a virtual visit seem like you are in person. This would look like checking in with somebody at the virtual front desk and having that person verify information and insurance, just as they would for an in-person visit. When the patient is “roomed” and confirmed to be online and ready, then the nurse and physician are brought into the video interaction. Once the session is established, the doctor can step in without having the burden of troubleshooting technology.
Creating telehealth workflows aligned to known processes similar to in-person experiences takes the burden off physicians and gives them a familiar workflow, ultimately boosting adoption.
By Keith C. Kosel, PhD, MHSA, MBA, vice president of enterprise relationships, PCCI.
Aligning groups that have very different backgrounds and agendas, for the good of the community, is no easy matter. Whether at the city, state, or federal level, governmental or civic entities are tasked with trying to build consensus among various stakeholder groups to affect an outcome that works for the constituents they represent. It is no different for those tasked with leading a Connected Community of Care (CCC).
The Role of Governance
The premise behind the CCC is that by bringing together healthcare providers, community-based social service organizations (CBOs), faith-based organizations, and various civic entities, a community can establish a network of care providers focused on addressing residents’ social and/or clinical needs. While the premise is straightforward, establishing the governance group and governance structure to set up and manage a CCC is anything but straightforward. Before we look at how we might bring entities with different missions and agendas to the table, let’s understand what we mean by a governance group and a governance structure, and why these are essential to form a successful CCC.
The nucleus of a CCC is its governance group? those organizations that have come together to establish the CCC and to form the rules by which it will operate (the governance structure). As most CCCs form from scratch, the governance group is typically made up of one or two organizations we refer to as Anchor Organizations. These are typically large, well-established, and highly respected organizations within the community.
They could include national social service organizations such as the United Way or Salvation Army, or they could be philanthropic funders, faith-based organizations or healthcare systems. What all these organizations have in common is a mission to improve the health and well-being of their community’s residents. As such they lie at the heart of the governance group (Figure 1).
Figure 1. Connected Communities of Care Including Governance Structure
In addition to the Anchor Organizations, the governance group typically consists of four to six additional Partner Organizations. These may be somewhat smaller CBOs (in scale and scope), but they all play a foundational community role in addressing resident’s social and/or clinical needs. Partner Organizations are well-known within the community and historically work closely with the Anchor Organizations. Partners could be regional food banks, housing assistance providers, crisis centers, mental health providers, local school districts, etc.? all defined by the fact they deliver essential social or clinical services within the community.
By Thomas Pace, vice president, global enterprise solutions, Blackberry Cylance.
Thomas Pace
Recently, hacking group Cozy Bear attempted to steal COVID-19 vaccine research from multiple organizations in Canada, the United States, and the United Kingdom. The hackers, reportedly under the employ of the Russian government, scanned targets for network vulnerabilities in an effort to infect them with network tracking and file exfiltration malware. This is not the first time research into the novel coronavirus has been a target and it is unlikely to be the last.
On some level, this news is unsurprising, as healthcare has always been an attractive target for cybercriminals.
Patient data is a valuable commodity on the black market, often containing everything one would need to know in order to commit various types of fraud. Access to critical systems can be a literal case of life and death, and these systems are often so interconnected that an attack may spread like wildfire. Finally, many healthcare agencies lack the time and resources to prioritize cybersecurity to the degree that they should.
Yet this is also a unique situation. We are currently in the midst of a global pandemic, a period of heightened sensitivity and unprecedented digitization. People in all industries are exhausted and anxious, a combination which makes them particularly susceptible to mistakes.
Moreover, vaccine research is a priority for governments across the world. Each seeks to lessen the virus’s impact on their citizenry and economy, with many employing state-sponsored actors to give themselves a leg up. Rank-and-file criminals, meanwhile, are also perfectly willing to exploit the situation for their own gain.
At all levels, phishing campaigns remain the number one attack vector. There’s no need to waste effort trying to break through an organization’s defenses if one can simply trick an employee into granting access. Agencies researching the COVID-19 vaccine are particularly susceptible to targeted phishing attacks due to the collaborative nature of their work.
By Richard Bailey, lead IT strategist, Atlantic.Net.
covered entity and a business associate. It is a HIPAA law created to ensure that all of the HIPAA compliance risks (administrative, physical, and technical) are identified, and a roadmap is designed to plan the fixes necessary to resolve the issues found.
The risk assessment was not part of the original Health Insurance Portability and Accountability Act of 1996. Instead, it was first introduced in the 2003 Privacy Rule and Security Rule amendments and was then further expanded upon in the Final Omnibus Rule of 2013.
HIPAA legislation defines a Covered Entity (CE) as anyone that handles PHI during day-to-day business operations. Most businesses working in the healthcare industry are considered Covered Entities.
The U.S. Department of Health and Human Services (HHS) officially defines a CE as; Healthcare Providers such as doctors, dentists, nursing homes, pharmacies, health insurance companies, HMOs, Medicare, Medicaid, and Clearinghouses.
A business associate is any third party business or organization that handles individually identifiable health data on behalf of a covered entity, and the risk assessment is often considered the starting point to achieve HIPAA compliance.
What is a risk assessment?
A risk assessment is commonly the first task undertaken when a covered entity and a business associate enter into Business Associate Agreement (BAA). Its purpose is to identify areas within the business that process, store, and transmit protected health information (PHI) that are in the scope of HIPAA compliance.
PHI is patient data that the law is meant to safeguard, such as data that can be used to identify an individual personally. Examples may include patient names, email addresses, social security numbers, insurance certificates, and so on.
Areas of risk are highlighted, and a roadmap is created for the CE to become HIPAA compliant. Most risk assessments follow the NIST cybersecurity framework, and the NIST schema is a straightforward but highly productive process. There are five essential parts of the NIST framework, and these are; Identify, Protect, Detect, Respond, and Recover. The OCR takes this further with the nine essential elements of Risk Analysis but either framework covers similar topics.
Q&A with Matt Fairhurst, CEO and co-founder, Skedulo.
Skedulo is a champion of the deskless workforce, providing a comprehensive productivity platform that improves the lives of the mobile worker. Operating heavily in the healthcare sphere, Skedulo works with home healthcare agencies and organizations including Solace Pediatrics, Eastseals, and New Jersey Respiratory Associates (NJRA). Matt Fairhurst is the co-founder and CEO of Skedulo. Matt’s background is in user experience and user interface design, and, from this, he has a passion for building great products. Here he discusses telehealth, technology innovation and the future of healthcare.
What’s been the experience of the practice or the health system with the technology, and how has its real-world application changed the way they practice or the business of care?
Telehealth is a positive development in the healthcare industry, one that, 20 years ago, people never thought would be possible. It allows patients to “visit” the doctor without having to leave their home via video chats, and it also enables caregivers to visit patients in their homes and still be able to complete the job efficiently.
Pre-pandemic, telehealth was often seen as a backup option for healthcare providers, for example if the patient lived elsewhere and was unable to come in for a physical appointment. Then once the pandemic hit, telehealth became the temporary default and was practiced out of necessity in order to limit potential contamination. Now, providers are beginning to think about how they want to incorporate telehealth into their regular model of care. Practicing telehealth is less expensive and allows more patients to be seen. While it won’t replace in-person care, it certainly will stick around once the pandemic passes and be incorporated into how healthcare systems practice their business of care.
Why were doctors and people reluctant to adopt telehealth prior to the pandemic?
The healthcare industry has always been resistant to adopting technology and interoperability, and that includes telehealth services. Many providers held on to the belief that virtual services were inadequate compared to in-person services. The silver-lining of COVID’s effect on healthcare is that it’s propelling the industry forward and forcing an openness to digital transformation. And technology — thanks to biometric devices and software innovation — is finally catching up to make telehealth a seamless and truly comparable option to certain in-person services.
Understanding the impact that Brexit can have on our way of life can seem very daunting at first, but when it comes down to the finer details such as the distribution of medication, there is a lot that could be about to change. In this article, we will be providing you with insight into how the pharmaceutical distribution process will be affected by Brexit.
Changes To International Regulations
When looking at the impact that Brexit can have on our lives in the UK at the end of this year can seem quite daunting at first. However, within the pharmaceutical sector, there is set to be the most amount of change. Not only are there changes to distribution itself, but there are also changes to international regulations that are set to revolutionize the distribution of medication and PPE between the UK and Europe. Though there has been nothing set in stone regarding these changes in regulation at this time, the end of the year could reveal a deal that has been made.
Trade of Pharmaceuticals with the EU
It is important to remember at this time that the UK has had a long history of trading with the EU for PPE and medication. Figures have shown that in 2016 alone the UK exported £24.9 billion in pharmaceutical goods. With Brexit however, this could be set to change as regulations and tariffs on trading goods could lead to a significant drop in the amount of revenue that the UK brings in every year.

 Aligning groups that have very different backgrounds and agendas, for the good of the community, is no easy matter. Whether at the city, state, or federal level, governmental or civic entities are tasked with trying to build consensus among various stakeholder groups to affect an outcome that works for the constituents they represent. It is no different for those tasked with leading a Connected Community of Care (CCC).
Aligning groups that have very different backgrounds and agendas, for the good of the community, is no easy matter. Whether at the city, state, or federal level, governmental or civic entities are tasked with trying to build consensus among various stakeholder groups to affect an outcome that works for the constituents they represent. It is no different for those tasked with leading a Connected Community of Care (CCC).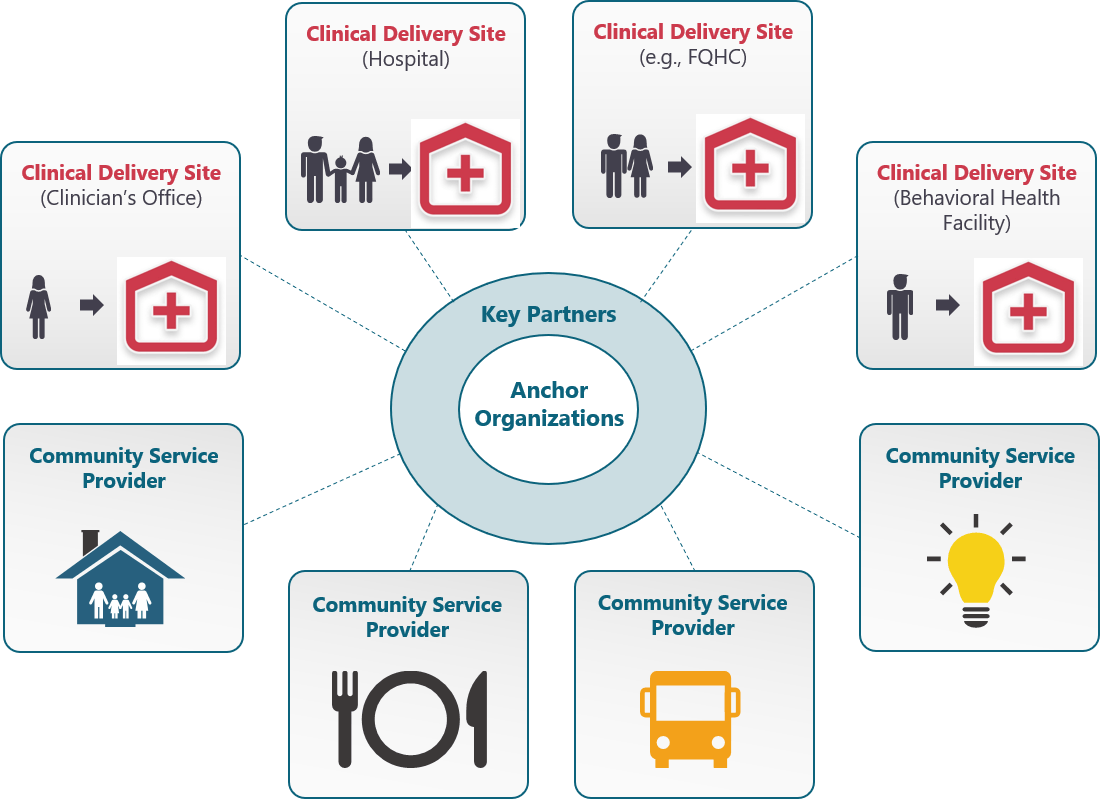

 Skedulo is a champion of the deskless workforce, providing a comprehensive productivity platform that improves the lives of the mobile worker. Operating heavily in the healthcare sphere, Skedulo works with home healthcare agencies and organizations including Solace Pediatrics, Eastseals, and New Jersey Respiratory Associates (NJRA). Matt Fairhurst is the co-founder and CEO of Skedulo. Matt’s background is in user experience and user interface design, and, from this, he has a passion for building great products. Here he discusses telehealth, technology innovation and the future of healthcare.
Skedulo is a champion of the deskless workforce, providing a comprehensive productivity platform that improves the lives of the mobile worker. Operating heavily in the healthcare sphere, Skedulo works with home healthcare agencies and organizations including Solace Pediatrics, Eastseals, and New Jersey Respiratory Associates (NJRA). Matt Fairhurst is the co-founder and CEO of Skedulo. Matt’s background is in user experience and user interface design, and, from this, he has a passion for building great products. Here he discusses telehealth, technology innovation and the future of healthcare.