(Connected Communities of Care Definition: An innovative method for effective population health management using social determinants of health. A way to streamline effective coordination between medical, government and community-based organizations.)
We ask this type of question every day. For example, we may ask? “Is this product that I purchased making a difference?” or “Is this advanced training that I completed making a difference?” Implicit in this common question is the expectation that because we have made an investment in something to achieve a result, the result should be better or more improved than the pre-investment state. So too with a Connected Community of Care (CCC).
As I have discussed in previous blogs, establishing a CCC requires a substantial investment in both time and money. Therefore, it is only natural to ask? “Is this CCC making a difference, and how would I know?” Unfortunately, most CCCs are established with very little forethought given to this exact question. While we expect the CCC will help community residents improve their health and well-being, how will we know conclusively that this has happened?
How will we demonstrate its impact to a potential partner or? more importantly? a funder? This is where data, measurement, and evaluation come into play. For most people, these three words cause anxiety levels to immediately rise. But this doesn’t need to be the case; a little planning and forethought can go a long way to assuaging one’ anxiety when asked the question, “Is your CCC making a difference?”
Before we think about what data we will need to answer this question or how we will collect it, we first need to establish what we mean by “making a difference”. Understand, there is no one correct answer to this question. What may constitute a positive difference or impact for one organization may be much different for another, even similar organization. Many factors contribute to the final answer and each are usually organization-, ecosystem- and situation-specific.
In practice, there are many ways to define making a difference. First, we can look at quantitative or numeric information to make this determination. Are we providing more nutritious meals to indigent residents? Is the number of inappropriate Emergency Department visits declining or, conversely, is the number of residents having visits with a primary care provider increasing? All of these effects can be counted and judged against some predefined goal (more on this later).
Second, we can assess making a difference by asking the people that are being touched by the CCC. Through surveys or brief interviews, community residents can tell you in their own words what impact, if any, the CCC has on their lives. While this qualitative (non-numeric) information can often be more informative than simple quantitative information because it represents the voice of the individual, to answer the question of whether your CCC is making a difference, you will also still likely need to establish numeric goals.
A third way to assess whether your CCC is making a difference is indirectly via the financial and non-financial opportunities that arise as a result of having a CCC versus not having one. For example, having a CCC may make it much easier to perform contact tracing among vulnerable populations during a pandemic like COVID-19. Having a CCC may also enable a healthcare system or a community-based organization (CBO) to apply for a grant that it otherwise might not be competitively positioned to do if it did not have an integrated system of healthcare and social service providers such as a CCC.
We’ve all experienced crises in our lives. They may be personal in nature (e.g., involving our interpersonal relationships), organizational (e.g., relating to our employment or retirement income) or nature-made (e.g., floods, tornados, or the COVID-19 pandemic). When crises hit our communities, the impacts can be widespread and far-reaching.
Healthcare providers and community-based organizations (CBOs) are called upon to provide more rapid and extensive care and support to the community than is otherwise the norm. A well-established and highly functioning Connected Community of Care (CCC), as is the case here in Dallas, Texas, can provide a tremendous strategic and tactical advantage over non-connected peers.
Since 2014, the Parkland Center for Clinical Innovation (PCCI) has led an effort to bring together several large healthcare systems and a number of regional social-service organizations such as food banks, homeless assistance associations, and transportation service vendors, along with over 100 smaller CBOs (i.e., neighborhood food pantries, crisis centers, utility assistance centers) and area faith-based organizations to form the Dallas CCC.
Over time, civic organizations, such as the Community Council of Greater Dallas, Dallas County Health and Human Services (DCHHS), and select academic institutions have begun to participate in various community-wide projects under the Dallas CCC umbrella. Central to the success of the Dallas CCC are the partnerships that have been formed between the CBOs and a number of local healthcare systems (Parkland Health & Hospital System [Parkland], Baylor Scott & White Health, Children’s Medical Center, Methodist Health System, and Metrocare Services), clinical practices, and other ancillary healthcare providers serving the Dallas metroplex. These partnerships have proved essential in building a truly comprehensive and functional network aimed at improving both the health and well-being of Dallas residents.
Connecting these various entities and forming a two-way communication pathway is an electronic information exchange platform termed Pieces Connect, which allows for real-time, two-way sharing of information pertaining to an individual’s social and healthcare needs, history, and preferences.
The information exchange platform is the glue that holds the physical network together and provides one of the mechanisms to disseminate information from public health and healthcare entities to social service providers in the community. It allows the individual community resident, via the CBO, to become better informed about important health issues, such as routine vaccinations or preventive care, such as social distancing and proper mask usage during a pandemic.
Until recently, the primary mission of the Dallas CCC focused on addressing residents’ social determinants of health (SDOH) issues through providing community resources (e.g., food assistance, housing, transportation) to improve the lives of Dallas County residents. While this mission has become even more critical during the COVID-19 pandemic, the work of the Dallas CCC has also evolved to include identifying COVID-19 sites within the County and directing community outreach efforts to help stem the rapid spread of the virus.
By Keith C. Kosel, PhD, MHSA, MBA, vice president of enterprise relationships, PCCI.
Aligning groups that have very different backgrounds and agendas, for the good of the community, is no easy matter. Whether at the city, state, or federal level, governmental or civic entities are tasked with trying to build consensus among various stakeholder groups to affect an outcome that works for the constituents they represent. It is no different for those tasked with leading a Connected Community of Care (CCC).
The Role of Governance
The premise behind the CCC is that by bringing together healthcare providers, community-based social service organizations (CBOs), faith-based organizations, and various civic entities, a community can establish a network of care providers focused on addressing residents’ social and/or clinical needs. While the premise is straightforward, establishing the governance group and governance structure to set up and manage a CCC is anything but straightforward. Before we look at how we might bring entities with different missions and agendas to the table, let’s understand what we mean by a governance group and a governance structure, and why these are essential to form a successful CCC.
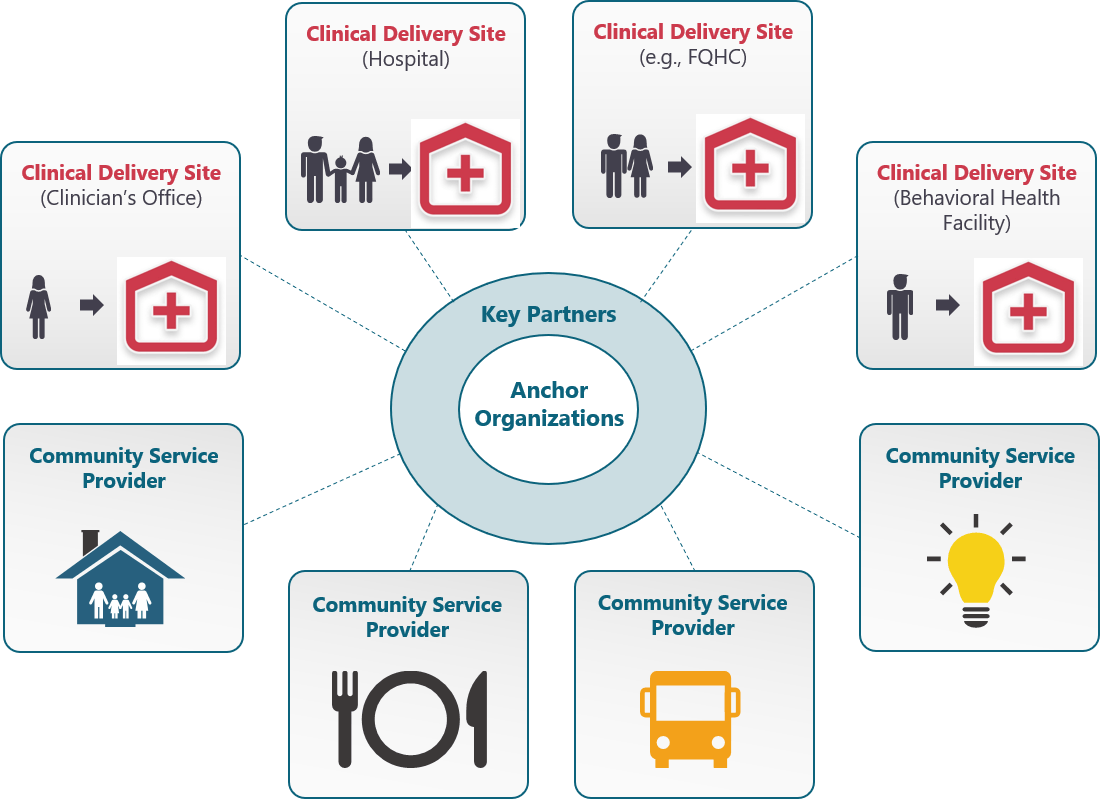
The nucleus of a CCC is its governance group? those organizations that have come together to establish the CCC and to form the rules by which it will operate (the governance structure). As most CCCs form from scratch, the governance group is typically made up of one or two organizations we refer to as Anchor Organizations. These are typically large, well-established, and highly respected organizations within the community.
They could include national social service organizations such as the United Way or Salvation Army, or they could be philanthropic funders, faith-based organizations or healthcare systems. What all these organizations have in common is a mission to improve the health and well-being of their community’s residents. As such they lie at the heart of the governance group (Figure 1).
Figure 1. Connected Communities of Care Including Governance Structure
In addition to the Anchor Organizations, the governance group typically consists of four to six additional Partner Organizations. These may be somewhat smaller CBOs (in scale and scope), but they all play a foundational community role in addressing resident’s social and/or clinical needs. Partner Organizations are well-known within the community and historically work closely with the Anchor Organizations. Partners could be regional food banks, housing assistance providers, crisis centers, mental health providers, local school districts, etc.? all defined by the fact they deliver essential social or clinical services within the community.
This question initially brings to mind many possibilities such as connection to the latest 5G cellular service, a new super-fast internet provider, or maybe one of the many new energy suppliers jockeying for market share from traditional utility companies.
While all of these might represent legitimate opportunities to improve one’s community, here we are talking about a different concept; specifically, whether your community is ready to have a Connected Community of Care (CCC) to advance whole person health.
The image of a CCC may seem obvious. After all, we all live in communities where we have some connections between hospitals, physician practices, ambulatory care centers, and pharmacies to name just a few. But here we are talking about a broader sense of connected community that includes not just healthcare organizations, but social service organizations, such as schools and civic organizations and community-based organizations (CBOs) like neighborhood food pantries and temporary housing facilities.
A true CCC links together local healthcare providers along with a wide array of CBOs, faith-based organizations and civic entities to help address those social factors, such as education, income security, food access, and behavioral support networks, which can influence a population’s risk for illness or disease.
Addressing these factors in connection with traditional medical care can reduce disease risk and advance whole person care. Such is the case in Dallas, Texas, where the Dallas CCC information exchange platform has been operating since 2012. Designed to electronically bring together local healthcare systems, clinicians, and ancillary providers with over a hundred CBOs, the Dallas CCC provides a real-time referral and communication platform with a sophisticated care management system designed and built by the Parkland Center for Clinical Innovation (PCCI) and Pieces Technologies, Inc.
Long before this information exchange platform was implemented, the framers of the Dallas CCC came together to consider whether Dallas needed such a network and whether the potential partners in the community were truly ready to make the commitments needed to bring this idea to fruition.
As more and more communities and healthcare provider entities realize the tremendous potential of addressing the social determinants of health by bringing together healthcare entities and CBOs and other social-service organizations, the question of community readiness for a CCC is being asked much more often. But how do you know what the right answer is?
Before looking at the details of how we might answer this, let’s remember that a CCC doesn’t don’t just happen in a vacuum. It requires belief, vision, commitment? and above all? alignment among the key stakeholders. Every CCC that has formed, including the Dallas CCC, begins with a vision for a healthier community and its citizens.
This vision is typically shared by two or more large and influential key community stakeholders, such as a large healthcare system, school district, civic entity, or social- service organization like the United Way or Salvation Army. Leaders from these organizations often initially connect at informal social gatherings and advance the idea of what if?
These informal exchanges soon lead to a more formal meeting where the topic is more fully discussed and each of the participants articulates their vision for a healthier community and what that might look like going forward. This stage in the evolution of a CCC is perhaps the key step in the transformation process, as while all stakeholders will have a vision, achieving alignment among those visions is no small feat.
Many hopeful CCCs never pass this stage, as the stakeholders cannot come to agreement on a common vision that each can support. For the fortunate few, intrinsic organizational differences can be successfully set aside to allow the CCC to move forward.