By Kali Durgampudi, chief technology, innovation officer, Greenway Health.
Kali Durgampudi
Like so many industries in today’s Third Industrial Revolution, the pace of innovation in healthcare today is fast and ever-changing. New technologies – like artificial intelligence (AI), machine learning, big data, the Internet of Things (IoT) and voice recognition – are at the heart of applications and tools that are becoming demanded by patients and more ingrained in clinicians’ daily workflows.
For vendors developing new solutions based on these technologies, it appears they find themselves in a ‘race,’ striving to be first-to-market in order to establish their competitive edge. But being on the bleeding edge of innovation isn’t always easy. The healthcare industry has not been immune to this rapid quest for first-mover advantage. Often when this occurs, these new solutions sacrifice the quality and functionality required to deliver on promised improvements.
Think about the initial introduction of the electronic health record (EHR). Billed as a way to make practices and physicians more efficient, many early EHR solutions had the opposite effect – creating a significant learning curve and adding to physicians’ workloads overall. While EHRs may have made great strides toward digitizing medical records, taking paper and manual processes out of the equation, they often created new problems that placed different burdens on practices, providers and patients. In fact, in the early days, physicians reported spending more than half of their workday – an average of six hours – using the EHR, plus another 86 minutes after hours.
But EHRs are not the only healthcare technology solution attributing to this challenge – it transcends innovation across the entire health IT sector. As an industry, we must take a step back and slowdown to ensure all new technology can deliver meaningful change to practices, providers and patients.
How to Design New Healthcare Technology with the End-User in Mind
A key to ensuring healthcare technology delivers true benefits is considering how it will fit into day-to-day operations of the end-user – whether that be a patient, a nurse, a surgeon or a billing manager. Before introducing any new technology to the market, make sure your first intention is to get it right.
To do that, engineering teams must employ “user-centered design,” a concept that emerged in the mid-1980s. This approach, defined by the International Standards Organization, “aims to make systems usable and useful by focusing on the users, their needs and requirements, and by applying human factors/ergonomics, usability knowledge and techniques.” The goal ultimately is to enhance effectiveness and efficiency, improve human well-being, user satisfaction, accessibility and sustainability, and to counteract possible adverse effects of use on human health, safety and performance.
User-centered design in healthcare could entail shadowing a nurse to observe his workflow when triaging patients, following a surgeon to see how she develops post-op papers, or interviewing patients to understand how they obtain healthcare information in their daily lives.
With that experience, you can then ascertain what capabilities would make users’ lives easier or more effective. From there, determine if there’s a way to improve an existing product on the market to fulfill needs, or whether a completely new platform is required.
Key Questions to Answer When Implementing a User-Centered Design Approach
There are several questions you must consider when following this method:
By Aaron Perreira, director of integrated marketing, Kareo.
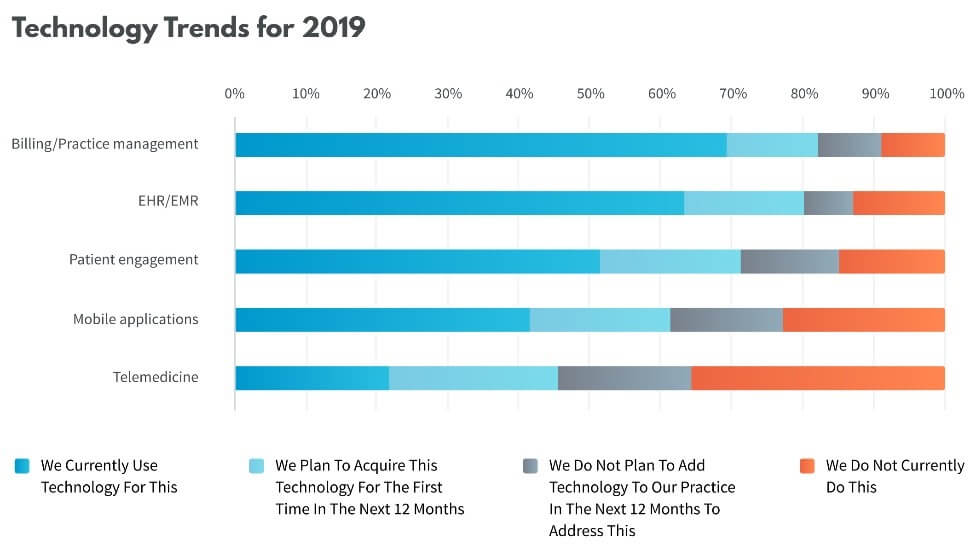
Over 70% of independent medical practices agree that the time demands of electronic health records (EHR) data entry detracts from care delivery. Simultaneously, 69% of independent practices state that integrated technology solutions are needed to improve the efficiency and profitability of their practices. This interesting “love/hate” relationship between independent practitioners and technology was shared in the recent 2019 State of the Independent Practice Industry Report, published by Kareo, a cloud-based medical software company.
The report was based on a nationwide survey designed to uncover the current challenges and expectations of independent practitioners in several areas of their practices, including care delivery, billing, patient engagement and regulatory compliance. Attitudes regarding the role of technology emerged in each of the areas surveyed.
Providers are increasingly reliant on their EHRs to manage their day-to-day clinical operations and maintain regulatory compliance. For many practices, the use of EHRs began when the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 was signed into law by President Obama on February 17, 2009. The HITECH Act was created to motivate the implementation of electronic health records by providing monetary incentives for being able to demonstrate meaningful use of electronic health records.
At that time, the market was flooded with more than 700 EHR vendors looking to capitalize on the EHR gold rush. Many practices adopted EHRs at that time, however since then, as the regulatory standards and consumer requirements for EHR technology continued to evolve, an increasing number of software providers have failed to keep up with technology and have fallen out of the race. This has left many providers tethered to antiquated, ineffective systems. More established practices (in practice for 10 or more years) appear to be more gun shy in that they likely adopted their EHR several years ago and had to suffer through poor implementations of costly but under-performing software that didn’t deliver on the value that was promised.
Despite government mandate, penalties and incentives, only 64% of respondents are currently using an EHR today. This low figure likely represents both the entry of newer practices that haven’t yet implemented their EHR platform and the fact that some practice specialties such as mental health, are more likely to still be using paper-based records and haven’t made the switch to electronic records.
Over the last few years, hospitals and healthcare practices throughout the country have started adopting new technology that helps them provide better care to their patients and make life easier for their employees.
For example, 64 percent of physicians now send electronic messages to their patients via text or email. Meanwhile, 63 percent allow their patients to view their medical records online.
Are you looking for new ways to bring your practice into the 21st Century? Listed below are seven of the top healthcare technology trends you ought to know about and consider implementing in your practice.
Electronic Medical Records
Electronic medical records (or EMR for short) are one of the most popular tech trends in the healthcare world.
Lots of practices have started using EMR to simplify the process of searching for patient records. EMR has also made it easier for patients to access their medical records online.
Even though plenty of practices are making use of EMR, there are still a lot of them that haven’t made the switch yet. The sooner you start making your files available in a digital format, the sooner you’ll start reaping all the benefits of EMR.
For example, EMR provides immediate access to patient records. It also helps physicians make better decisions about their patient’s care.
They can spot patterns more easily when everything is in front of them. This, in turn, allows them to choose the best treatment approach and avoid missing something important.
Blockchain Technology
Blockchain has started to make its way into the healthcare world, and it’s not showing any signs of leaving.
Blockchain technology allows healthcare practices (and other businesses, for that matter) to store digital information without taking up a ton of space. It also allows them to store their information in a more secure way since it cannot be copied.
In the digital age, patient security and privacy protection are of the utmost importance to many healthcare professionals.
Blockchain systems allow practice owners and managers to ensure they’re keeping patient records and information safe. It also helps them to avoid expensive and harmful (on many levels) data breaches.
Telemedicine
In 2019, many people are looking for new ways to get things done without leaving their homes. They have groceries delivered to their door, for example, and they communicate with friends and family via video chat.
Lots of healthcare practices are jumping in on this trend and are making it easier for patients to have their medical needs met from the comfort of their own homes as well.
Telemedicine allows patients to talk to doctors, receive medical advice, and even have prescriptions filled, without having to make a special trip to the doctor’s office.
Physicians are also using these same technologies to communicate with each other in more effective ways and come up with better, more comprehensive solutions for their patients.
Artificial Intelligence
Artificial intelligence is for way more than gaming. It’s also one of the biggest healthcare trends of 2019.
Physicians and researchers have started or have plans to start using artificial intelligence in a variety of ways.
As artificial intelligence technology becomes more refined, it will be easier for healthcare professionals to monitor their patients and provide better diagnosis and treatment.
It will also likely enhance the telemedicine world as well, as it will make it easier for physicians to see their patients without having to be in the same physical location as them.
Wearables
Wearable health monitoring devices are not new. However, they’ve become more popular than ever, and they’re also becoming more advanced.
As these devices become more accurate and able to provide more details about the wearer’s health, it’s likely that many physicians will start relying on them to gather information about their patient’s health and daily habits.
As provider adoption of electronic health records (EHRs) approaches near-universal levels, a study from The Doctors Company shows the frequency of claims in which EHRs contributed to injury continues to rise.
Analyzing EHR-related medical malpractice claims that closed between 2010 and 2018, The Doctors Company uncovered that the pace of these claims tripled, growing from a mere seven cases in 2010 to an average of 22.5 cases per year in 2017 and 2018.
While EHRs are not often the primary cause of claims, the study shines a light on potential risks they may pose in care delivery, as well as the top factors that contributed to the claims. The study showed that EHR-related claims were caused by either system technology and design issues or by user-related issues. Among the top findings:
Top user-related issues stem from incorrect information, pre-populating or copying and pasting, and hybrid health records or EHR conversion.
Top system technology and design issues were problems with electronic systems and technology failure.
Of those injuries that occurred in 7 percent or more of claims, adverse reaction to a medication and death were by far the most prevalent.
Diagnosis-related allegations represented nearly one-third of the total.
Two specialties—family medicine and internal medicine—received the highest percentage of claims where EHRs are a factor, followed by cardiology and radiology.
Based on this data, study author Darrell Ranum, JD, CPHRM, vice president of patient safety and risk management at The Doctors Company, identified the following steps to prevent EHR-related risks that may ultimately contribute to an adverse event:
EHR general dissatisfaction is well-known. Despite how hard electroni? patient records can be to use, a number of doctors are saying the technology has made them better caregivers.
Our friends at Belitsoft (a medical software development company) have brought you answers to some important questions. Why do physicians prefer using EHRs and how this technology improve their workflow? What EHR features make doctors keep up to date? Read on to find out!
Quick access to comprehensive medical records
EHR is advocated as a doorway to smarter and more accessible healthcare. The Surescript report found that one-third of surveyed can easily determine which other care providers a patient has visited. Specialists are able to compile a comprehensive patient history by using any hit found in their records.
“Having real-time access quickly and reliably to medical information and data 24/7 is important to make this happen. Instead of hunting for lab work in a paper chart or trying to find a specialist’s consultation, I can access the information I need rapidly and focus on the patient in front of me.”
It is usually hard to detect common hospital-acquired infections in a crowded building where patients might get infected at every turn. The research published in JAMA Internal Medicine, “is a brilliant example of how we can learn from data in the electronic health records,” said Robert M. Wachter, MD, professor and chair of the Department of Medicine at UCSF.
The idea belongs to the UCSF Health Informatics team. They realized that each patient’s EHR contains detailed info about every step they had made for every test. Using these digital breadcrumbs found in the records, specialists were able to track patients in time and space, thus discovering a significant source of infection.
Dr. Jen Gunter supports EHR implementation and says she really loves the system. One of the features Jennifer highlights is a full integration with pharmacy services.
She has noted that many patients can’t remember their medications or doses, and even go off the meds she prescribed. Thus, for example, Dr. Gunter can take a guess and potentially have a patient buy an expensive medication.
Alternatively, she can call the pharmacy (if she remembers which services she used) to see if they can track down the right medication history and then she or her nurse appoints a follow-up visit if they get the answer.
However, the only viable option for Dr. Gunter is to use an EHR system. Thus, she can confirm the info with the electronic records and talk with a patient about how and why deviations happened.
By Adarsh Jain, editor, Transparency Market Research.
Timely diagnosis and advanced treatment measures are imperative for better healthcare outcomes. But, little have we realized the criticality of patient’s history in treatment. It is human to remember information about major healthcare incidents, but it is impossible for individuals to store every detail of medical history. And sometimes, the lack of details on medical history can be the difference between life and death.
Over the years, as information technology and computers began finding applications in healthcare diagnosis and treatment, it is also emerged as a critical tool to store and retract data. Synonymous to a business, where all major decisions are data-driven, healthcare providers, too, realize the need for data on patient’s health to decipher treatment and diagnosis. As we realize the potential for big data analytics across industry verticals, cloud computing has enabled tech giants develop tools that could come in handy in critical situations. Transparency Market Research states that the global electronic health records market stood at $3,225 million in 2016, and predicts that it will grow to $38,278 million by the end of 2025.
Electronic Health Records are Older than the Internet
It was in 1960s, three decades before the internet bubble, when attempts were made to introduce electronic health record systems. Larry Weed first developed a system to record problem-oriented health records. And, in 1972, Regenstrief Institute, developed a possible system to record health data electronically. However, huge cost and lack of feasible infrastructure remained an impediment to electronic health record tools.
Things began to change at the turn of the century when internet became a phenomenon, and tech companies began sensing the need for data-driven approach for every business. In short order, tech giants – from Google to everyone else — started working to develop products for electronic health records.
North America At the Forefront
It is, perhaps, safe to state that U.S. is at the top when it comes to healthcare infrastructure. With consistent financial and policy-level support from the U.S. government, and conducive environment for pharmaceutical, medical devices, and the IT industry, the region has leaped miles ahead from others. And, electronic health records is no different. Out of the $23,225 million reaped by the global electronic health records market, more than 46% came from North America.
While the overall market share for North America is expected to dip marginally by 2% by 2025, TMR analysts predict that it will continue to hold a mammoth share of growth in the eight-year-forecast period. Of the $15,000 million growth potential, North America alone is expected to garner $6,000 million.
How Government Policies Made a Difference?
The market for electronic health records in North America owes a large share of its success to favorable government policies. From Presidents George W. Bush to Barack Obama, each have introduced policies, set up bodies, and funded projects that have today, led to a robust set up for electronic health records in the U.S. It was in President Bush’s regime that the first move to improve healthcare IT became evident. With budget for the sector doubled, the Bush government also introduced an exclusive position in the cabinet for the National Health Information Coordinator. Further, the government under Bush also set 2014 as the deadline to adopt electronic health record systems. Taking cues from here, the Obama government too increased funds for initiatives promoting implementation of electronic health record systems.
The Influence of IT Infrastructure
Most tech giants in the world are headquartered in the U.S. and this provides North America the advantage over other regions. With conducive environment created by the government, there is little for tech giants to worry about. And with history for electronic health records born in the country, the spirit for developing products has always been higher in the region. Efforts are underway to soon launch products that could change the approach of healthcare in the country, and attempts look ripe to expand the efforts globally. A fallout of the efforts in the U.S. is taking shape in Asia Pacific, where both government, and business organizations, have begun taking baby steps in moving towards a future in electronic health records.
Healthcare is one of the fastest-growing segments of the digital universe, with data volumes expected to grow by 48 percent annually. Healthcare applications will be the principal driver of this data growth, with EHR penetration in the US already reaching more than 80 percent and expected to reach 95 percent by 2020.
In addition, the healthcare space has matured to the point where EHR replacement has become commonplace, and up to 50 percent of health systems are projected to be on second-generation technology by the year 2020.
So why are these data points an important consideration?
Healthcare organizations have been facing
the major challenge of storing and securing patient information. This is not
just the problem with the providers, but for payers and patients too. While
transitioning to complete digitization of practices, healthcare leaders,
specifically CIOs, often find it a daunting task to identify the areas where
they need to scale up their technological approach.
EHRs are likely the necessary evil for
healthcare. No doubt they solved so many problems; however, they opened gates
to other problems. The complications with the legacy systems compel hospitals
to shift to modern technological solutions.
Right now, the story of mergers and acquisitions in the space is also like an adventure movie. According to KLAS Research, the number of EHR vendors dropped from more than 1,000 to around 400 now — the reason being the rise in mergers and acquisitions.
Where does the actual problem lie?
The journey of shifting from legacy systems
to advanced technology is also ripe with its own set of complications. As the
landscape is molded by M&As, consistent EHR replacements are not rare
sights.
In this scenario, organizations face two
major problems:
Legacy systems have
to be maintained so that organizations are able to access the read-only PHI.
The cost of
migrating data from one EHR to another is unreasonably high.
Moreover, since these EHR replacements are directly linked to the retention of the data from the legacy systems for about a decade. Most states require Protected Health Information (PHI) to be retained for about seven to 10 years.
How is data archival the solution we need now?
Transitioning between EHRs require a
holistic approach to keep their data secure, and the best way here is data
archival. Data archival is a simple process of archiving the entire data from
legacy systems into a unified platform so that it can be kept secured for a
long duration. It is the perfect solution to the above-stated two problems: it
is easier and can be done at one-tenth of the price.
For instance, in the case of legacy systems, the EHR vendor can charge up to $10,000 a month for keeping the system running even after the transition. However, in the case of data archival, this entire process is fast, cheap and much more efficient. Also, it eliminates the necessity of keeping the legacy systems running.
The archiving process serves multiple
functions and has the following major advantages over other data-retention
processes:
It allows legal
decommissioning of the legacy systems
It ensures the
integrity of the vital healthcare data
It creates the
opportunity to realize opportunities for immediate Return on Investment (ROI)
It minimizes the
risk of maintaining the historical data
It develops a
centralized repository for all your legacy systems’ data
And many more …
What is the perfect data archival strategy?
The procedure of data archival mainly
consists of two major steps: identifying the need for data archival and
adopting the best archival solution. It is important to analyze the need first
and then take action. It is a complex process and involves complex compliance
requirements to be fulfilled.
So what is needed to be done now? Here is the list of essential prerequisites to be considered and followed religiously before archiving your crucial healthcare data:
Understand your healthcare data
The first step is to understand your EHR and legacy system data. One organization might be focusing on archiving the data from a single EHR while the other might be looking for a solution that can archive the data from multiple data sources. Everyone’s data needs are different and, thus, requires a different data archival approach.
Familiarize yourself with your state regulations
Every state has its own regulations to archive the data. The state of California might need you to archive your data for six years, while the state of Minnesota might have a span of more than 30 years. These regulations need to be considered and understood efficiently before investing in a data archival solution.
Chalk out your technological requirements
The next and
most important step is to identify the extent and the varieties of
technological features your organization might need. Every organization has
different needs which should be analyzed and understood well in advance. Based
on these insights, the final decision can be made about any data archival
solution and its abilities.
The road ahead
The space of healthcare is among the most diverse and ever-changing fields. New mergers, efforts towards making the practice data-driven, empowering providers with access to every single bit of data about their patients, and whatnot; these factors have compelled organizations to keep shifting towards a better option — a better EHR. And in this story, the ultimate goal is to make this transition as smooth as possible. It is important to ensure that organizations get rid of all their legacy system headaches instantly. With data archival, it is finally possible.
Most of us know someone who has been diagnosed with cancer and understand first hand the tidal wave of emotions and questions that come immediately after diagnosis. One question that sticks out to providers is the seemingly simple: “How many patients have you seen who are just like me?” and perhaps even more important: “Why are you confident that I can reach the magical five year survival rate?”
Unfortunately, with systems of record like the electronic health record, neither of these questions is easy for the provider to answer. The challenge is, in today’s oncology world there is both a combination of clinical confidence based on peer-reviewed data and the artistic necessity to understand what could work based on perceived comparable patients. Oncologists do incredible work to save lives, however, there is more to be done to help support the people who are making the most important decisions at the most critical inflection points.
Meaningful data to improve cancer care
Prior to the creation of EHRs, physicians stressed that they did not have enough access to data. While data is now being stockpiled within the depths of EHRs, physicians still do not have access to everything the data has to offer. The available data in EHRs is often fragmented, disorganized, and sometimes simply incomplete, making it difficult to glean any real value from this information after it is collected.
Essentially, the EHR can be compared to a messy bureau in your bedroom. While bureaus are intended to organize your clothes — socks in one drawer, t-shirts in another, etc. — sometimes socks windup in the pants drawer. All of the valuable information and data is in the EHR, but is sometimes lost in the wrong “drawers,” making it hard for clinicians to find the important information and make sense of it to impact patient care. While physicians are doing the best they can by adding information into EHRs, technology has not caught up to allow physicians to extract insights and put that data to use.
Fortunately, with the use of outside technology, we can pull real-world data (RWD) and real-world evidence (RWE) from the EHRs. This can unlock the insights hidden within the available data and uncap the potential for improving and personalizing cancer care, while reducing overall costs.
Unlocking hidden insights
The technology available today knows how data should be arranged. It knows when something is misplaced, and knows how to make sense out of it. Through advanced algorithms and clinical input, technology can essentially sort and gather RWD from EHRs and then group together similar patients based on their own biology, disease states, and other phenotypic factors, allowing for insight into treatment plans and potential outcomes.

 Providers are increasingly reliant on their EHRs to manage their day-to-day clinical operations and maintain regulatory compliance. For many practices, the use of EHRs began when the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 was signed into law by President Obama on February 17, 2009. The HITECH Act was created to motivate the implementation of electronic health records by providing monetary incentives for being able to demonstrate meaningful use of electronic health records.
Providers are increasingly reliant on their EHRs to manage their day-to-day clinical operations and maintain regulatory compliance. For many practices, the use of EHRs began when the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 was signed into law by President Obama on February 17, 2009. The HITECH Act was created to motivate the implementation of electronic health records by providing monetary incentives for being able to demonstrate meaningful use of electronic health records. Over the last few years, hospitals and healthcare practices throughout the country have started adopting new technology that helps them provide better care to their patients and make life easier for their employees.
Over the last few years, hospitals and healthcare practices throughout the country have started adopting new technology that helps them provide better care to their patients and make life easier for their employees.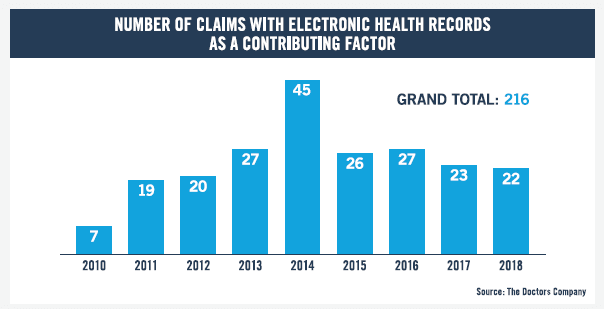 Analyzing EHR-related medical malpractice claims that closed between 2010 and 2018, The Doctors Company uncovered that the pace of these claims tripled, growing from a mere seven cases in 2010 to an average of 22.5 cases per year in 2017 and 2018.
Analyzing EHR-related medical malpractice claims that closed between 2010 and 2018, The Doctors Company uncovered that the pace of these claims tripled, growing from a mere seven cases in 2010 to an average of 22.5 cases per year in 2017 and 2018. Timely diagnosis and advanced treatment measures are imperative for better healthcare outcomes. But, little have we realized the criticality of patient’s history in treatment. It is human to remember information about major healthcare incidents, but it is impossible for individuals to store every detail of medical history. And sometimes, the lack of details on medical history can be the difference between life and death.
Timely diagnosis and advanced treatment measures are imperative for better healthcare outcomes. But, little have we realized the criticality of patient’s history in treatment. It is human to remember information about major healthcare incidents, but it is impossible for individuals to store every detail of medical history. And sometimes, the lack of details on medical history can be the difference between life and death.