By David Shelton, chief executive officer, PatientMatters.
More than half of Americans have experienced the sick feeling that comes with opening a medical bill they assumed would be covered by insurance. Surprise medical bills are on the rise, often driven by services administered at an in-network facility using out-of-network providers.
A Journal of the American Medical Association(JAMA)analysis of privately insured patients showed that between 2010 and 2016, inpatient admissions with an out-of-network bill increased 16%, and emergency department (ED) admissions with out-of-network billing went up more than 10 percent.
As alarming as the number of surprise bills is the impact on patients’ pocketbooks. In the same timeframe, potential patient liability skyrocketed from $804 to $2,040 for inpatient services and from $220 to $628 for ED visits.
Price transparency and accurate estimates are critical to preventing surprise bills and giving patients more control over their healthcare spending. Many providers are experiencing increases in self-pay patients, often because patients have a high-deductible plan that requires significant out-of-pocket before coverage kicks in. As such, patients need the ability to compare prices across providers and get accurate estimates of what they’ll owe before making healthcare decisions.
Why healthcare bill estimates are so difficult
Many factors contribute to the historical absence of bill estimates, but it starts with healthcare payment system fundamentals. Unlike other industries where transactions involve a buyer and a seller, healthcare brings in a third party, the payer, who is typically reluctant to reveal publicly what they pay various providers for services. Contracts, discounts, coding and other variables make it inherently difficult to achieve price transparency.
Price transparency progress
A step toward more price transparency came when the Centers for Medicare & Medicaid Services (CMS) required hospitals to publish their chargemasters online, starting January 1, 2019. Unfortunately, neither consumers nor many hospital employees could translate the data into usable, patient-specific bill estimates. In fact, more than half of hospitals in a 2019 survey said the move created further confusion.
In June 2019, President Trump issued an Executive Order to improve healthcare price and quality transparency. CMS later issued a final rule expanding current requirements for hospitals. These include providing a machine-readable file containing negotiated rates for all items and services annually and a consumer-friendly display of gross and negotiated rates for 300 “shoppable” items and services, including 70 defined by CMS. Insurers would also be required to provide members personalized out-of-pocket costs for all covered services in advance. These new rules are planned to take effect Jan. 1, 2021.
By Kali Durgampudi, chief technology, innovation officer, Greenway Health.
Kali Durgampudi
The electronic health record (EHR) industry continues to undergo a significant transformation, with many physicians asking themselves whether they consider their EHR a friend or a foe.
In too many cases, medical staff feel their EHR works against them, not for them. In fact, according to Medical Economics’ 2019 EHR score report, 60% of physicians said their current EHR system was harming their ability to engage with patients. In addition, The National Academy of Medicine found that as many as half of American physicians and nurses experience substantial symptoms of burnout. And, the same study found that poorly designed technology is a major contributing factor due to the increased amount of time needed to keep systems properly updated.
This should not be the case, and it’s time to change this narrative.
As we near a new year and a new decade, it’s time to focus on advancing EHRs to make the lives of physicians easier, while assisting in improving the patient experience, increasing engagement, enhancing administrative burdens, and more.
Required features and functionalities of EHRs in the next decade include:
Adaptability
Legacy EHR’s are typically thought of as outdated and lacking customization. Custom forms take months to build, cost extra and users ultimately lack control over the functionality. This is not acceptable by today’s standards. Every healthcare practice and specialty is different. So, the EHR must be customizable to fit each practices’ needs in order to optimize efficiency in data entry and management.
In addition, medical trends and challenges are constantly evolving. For example, opioid addiction has risen to epidemic levels in the United States, with the Centers for Disease Control and Prevention (CDC) estimating that more than 130 people die from an opioid overdose every day. Fortunately, health information technology has emerged as a powerful tool for tracking prescription activity.
EHR’s hold a tremendous amount of data – data that can help physicians provide better care to a specific patient or population. Armed with these analytics, a practice can gain insight into population health — along with reporting requirements for government incentive programs and data to optimize billing and cash flow.
According to the CDC, six in 10 Americans live with a chronic condition such as heart disease, cancer, or diabetes, and about seven in 10 deaths each year are due to a chronic condition. Through its analytics capabilities, a population health management solution can help a practice determine its highest-risk patient groups, identify gaps in care, and reach out to patients to engage them in their care.
The EHR of the next decade should be a tool for decision making. EHRs need to utilize advanced artificial intelligence (AI) and machine learning to make smart suggestions based on data.
An EHR should not just track if a patient is following their care plan, but alert providers when a patient has missed certain critical elements and make suggestions on how best to proceed. As such, the technology can be used to play a larger role in lowering no-show rates and helping predict which patients will have the most success – or biggest challenges – with certain treatment plans.
EHR’s should also be capable of helping physicians make the best financial decisions for their practices. In addition to increasing practice efficiencies and costs, EHRs assist in offering reduced drug and treatment plans with expected costs.
Healthcare is home to some of the most mind-blowing technological advances when it comes to diagnostics and therapies. At the same time, the healthcare system is responsible for many of the most head-scratching operational difficulties related to standard IT processes, such as those involved with moving data from one system or site to another. The same industry that successfully deploys remote-controlled surgery robots to heal a patient also struggles to send a discharge summary to a physical therapist for the same patient.
How can we explain this apparent paradox?
A Model of Interoperability
The simple answer is that interoperability in healthcare is a journey, not a destination. The question “why haven’t we solved interoperability?” assumes that interoperability is a one-time problem, when in fact the systems, standards, and data flows that constitute interoperability are constantly changing as the underlying patterns of treatment and reimbursement change.
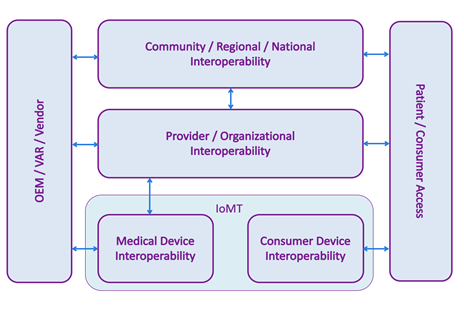
Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine[1].
In the center, provider, or organizational, interoperability indicates data flows within a single organization, typically a hospital or hospital system. This has historically been dominated by HL7 v2 transmitted over a TCP connection on a private network, although other standards and technologies are also used.
At the top, community, regional, and national cross-organizational Interoperability refers to communication of healthcare data across different organizations, for example ACOs, HIEs, and provider-to-payer data flows. In this part of the model, we often see IHE style integrations that exchange entire patient records in a single, secure transaction over a public network.
At the bottom, the Internet of Medical Things (IoMT) is divided into two parts: medical device interoperability, which concerns devices used in a clinical setting, and consumer device interoperability – commercially available devices marketed directly to consumers, such as fitness devices and in-home monitors.
On the left, healthcare IT vendors need to enable their products to interoperate at different levels of the interoperability model, depending on which markets they serve. For example, an EHR vendor will need its product to send and receive HL7 v2 messages in order to participate in the organizational interoperability space.
On the right, we are seeing an increased demand for patient or consumer access to their data, whether it is from a fitness device, a hospital’s EHR, or a payer’s disease management system. Integration in this box is often accomplished using APIs, including FHIR.
DirectTrust announces its Second Annual DirectTrust Summit, scheduled at the Washington Marriott Georgetown in Washington, DC, June 9-10, 2020. DirectTrust also announced its call for speaker proposals is now open to health information industry experts interested in speaking at the Summit.
DirectTrust is a nonprofit healthcare industry alliance created to advance the electronic sharing of protected health information (PHI) between provider organizations, and between providers and patients, for the purpose of improved transitions of care, care efficiency and coordination, patient satisfaction and reducing healthcare cost.
The DirectTrust Summit brings healthcare industry leaders together to share ideas and best practices around improving health information exchange and interoperability. In response to feedback from the inaugural summit this past June, the format for the Second Annual DirectTrust Summit has been expanded to include a full-day event on June 9 and a half-day of breakout sessions on June 10. Additionally, a virtual participation option via webcast is available for the full-day event and plenary sessions.
“We’re thrilled to announce the Second Annual DirectTrust Summit—and excited to be convening in Washington, DC,” said Scott Stuewe, DirectTrust president and CEO. “Our inaugural event in June was a terrific success, which is amply validated by the calls for more time and more sessions.
“As introduced, our intention with this Summit continues to be to look to the future; to build awareness and understanding of the many elements involved in and influencing the electronic sharing of health information, and to foster collaboration between DirectTrust members and DirectTrust members with non-members. Our goal is to help advance the industry’s progress toward achieving secure exchange among provider organizations, and between providers and patients nationwide,” Stuewe continued.
“With this in mind, we’re eager to learn about and share new and original applications of Direct Secure Messaging and interoperability, and invite industry experts to share their submissions on our Call for Proposals link,” concluded Stuewe.
This year’s Summit also adds a host committee responsible for evaluating speaker proposals and driving awareness of the event.
Members of the Host Committee were selected for their distinguished positions in healthcare interoperability. They include:
Jodi G. Daniel, JD, Partner, Crowell & Moring;
Leslie Kelly Hall, Founder, Engaging Patient Strategies and Consulting Executive, LifeWIRE Group;
David Kibbe, MD, MBA, Principal, The Kibbe Group;
Steven Lane, MD, MPH, FAAFP, Clinical Informatics Director, Privacy, Information Security, and Interoperability as well as a family medicine physician with Sutter Health;
Micky Tripathi, President and CEO, Massachusetts eHealth Collaborative
The Summit is open to both DirectTrust members and non-members. Additional information about the Summit—including Registration, Early Bird pricing, and Call for Speaker Proposals—may be found at bit.ly/DTSummit2020.
By Eric Hamborg, co-founder and chief commercial officer, MOBE.
Last month, I was honored to join some of the country’s most elite healthcare executives at the Health Care Executive Group Annual Forum – a closed-door forum to engage in in-depth discussions about challenges and opportunities facing the healthcare industry today. It’s an event I look forward to every year as we discuss pressing issues and how we can better collaborate across the industry to drive meaningful change and innovation.
Each year, the event culminates with a Top 10 list of challenges, issues and opportunities that HCEG members and forum attendees are expecting to confront in the coming year. Over 100 execs from the country’s leading healthcare organizations all worked together to develop this predictive list – debating, ranking and voting on 25 topics compiled from webinars, round tables and the 2019 Industry Pulse Survey.
As a co-founder of MOBE, I could relate to many of the Top 10 issues – they’re the challenges we grapple with every day as we bridge the gap between lifestyle choices and medical care in order to support individuals in achieving their best health outcomes. While the full list included several important topics, there were a couple that continually came up in my conversations with other executives at HCEG, and seem to be particularly important as we consider the needs of today’s healthcare consumer and the industry’s future:
Cost and Transparency
Healthcare costs continue to soar and consume 15% to 20% of the U.S. GDP, so it’s not surprising to see “Cost & Transparency” ranked first on the Top 10 list for 2020. Anytime we discuss challenges or innovation in the healthcare space, cost will remain central to the conversation.
The U.S. has the highest unit costs for nearly all services and procedures – yet we’re not even in the top 10 countries for health outcomes. Why the disconnect? This is the point where healthcare executives, news outlets, and politicians might start pointing fingers at each other. However, HCEG proved to be a venue for diverse thoughts and provoking conversations, arriving together at the core of our most imperative issues and what it will take to pursue progress. In all of my conversations, one word continually came up: transparency.
Although transparency alone won’t solve our cost problems, it’s a key part of the solution. At MOBE, we’ve found this can be particularly powerful for individuals in a hidden population with high-deductible plans, who make up 15% to 20% of the healthcare spend within our clients’ commercially insured populations. Promoting transparency from all corners of the industry will help to equip the consumer with the information they need to make better healthcare decisions.
Holistic Individual Health
Most exciting to my colleagues and me was seeing holistic individual health make it on the top 10 – an encouraging signal that we are on the right path here at MOBE. Throughout the forum, healthcare executives repeated the need for identifying, addressing, and improving an individual’s overall well-being in order to promote a frictionless and connected healthcare experience.
CAQH CORE and Health Level Seven International (HL7) announce a collaboration to address long-standing healthcare industry challenges by accelerating automation and improving interoperability between administrative and clinical systems. This is the first time these two organizations, which conduct complementary work to improve the electronic exchange of data across the healthcare industry, have collaborated on solutions to specific technical and administrative burdens.
“Our collaboration will help move the healthcare industry towards greater automation and streamlined business processes,” said April Todd, senior vice president, CAQH. “We are delighted to work with HL7 to address some of the biggest interoperability issues facing the industry.”
The two organizations will initially collaborate in three areas:
Prior Authorization: Currently, the prior authorization process is a labor intensive, time consuming, and costly administrative burden for providers and payers. It also frustrates patients and, in some cases, delays care. HL7 and CAQH CORE will collaborate to move the industry towards end-to-end automation of the prior authorization process.
Exchange of Medical Documentation: According to the CAQH Index, 84 percent of attachments, or documents that prove medical necessity, are exchanged manually and often contain too much, too little, or the wrong type of information. This delays prior authorizations, hinders the transition to value-based payments, and costs plans and providers time and money. HL7 and CAQH CORE will work to align their respective efforts to support the electronic exchange of clinical information and medical documentation.
Value-Based Payments: The transition to value-based payment models has been slowed by a patchwork of administrative and technical approaches and work-arounds. HL7 and CAQH CORE will work together to address the interoperability challenges causing administrative burden for innovative payment models.
“HL7 and CAQH have made great strides to improve the exchange of information in the healthcare continuum,” said Charles Jaffe, MD, PhD, CEO, HL7 International. “Our collaboration will enable better alignment and accelerate progress toward interoperability between clinical and administrative systems.”
The American Health Information Management Association (AHIMA) sent a joint letter to Congressional leaders today voicing concerns that certain provisions of the Office of the National Coordinator for Health Information Technology’s (ONC’s) recent 21st Century Cures Act (Cures) proposed rule on information blocking jeopardizes goals to foster a healthcare system that is interoperable, patient-engaged and reduces burdens for those delivering care.
The letter, co-signed by seven organizations representing the nation’s clinicians, hospitals, health systems and experts in health informatics and health information management, outlines several recommendations aimed at furthering the objectives of Cures, while ensuring that the final regulations do not unreasonably increase provider burden or hinder patient care.
“We support the intent of the Cures Act to eradicate practices that unreasonably limit the access, exchange and use of electronic health information for authorized and permitted purposes that have frustrated care coordination and improvements in healthcare quality and efficiency,” said AHIMA CEO Wylecia Wiggs Harris, PhD, CAE. “However, in light of the lessons learned from the meaningful use program, we believe it is crucial that we get this right. We look forward to discussing the details of these recommendations with congressional staff and ONC.”
Recommendations outlined in the letter include:
Additional rulemaking prior to finalization: ONC should seek further input from impacted stakeholders on issues including modifying the information blocking proposal to ensure that the requirements and exceptions are well-defined and understandable, and clinicians, hospitals and health information professionals are not inappropriately penalized if they are unable to provide a patient’s entire electronic health information through an application programming interface (API).
Enhanced privacy and security: The proposed rule does not sufficiently address Cures’ directives to protect patient data privacy and ensure health IT security. It is imperative that the Committee continues its oversight of privacy and security issues that fall outside of the Health Insurance Portability and Accountability Act (HIPAA) regulatory framework. This includes ensuring certified APIs include mechanisms to strengthen patients’ control over their data—including privacy notices, transparency statements and adherence to industry-recognized best practices.
Appropriate implementation timelines: ONC should establish reasonable timelines for any required use of certified health IT (CEHRT). Providers must be given sufficient time to deploy and test these systems, which must take into account competing regulatory mandates.
Revised enforcement: The U.S. Department of Health and Human Services should use discretion in its initial enforcement of the data blocking provisions of the regulation, prioritizing education and corrective action plans over monetary penalties.
For additional information on these recommendations, click here.
Signatories of the letter include:
American Health Information Management Association (AHIMA)
American Medical Association (AMA)
American Medical Informatics Association (AMIA)
College of Healthcare Information Management Executives (CHIME)
Federation of American Hospitals (FAH)
Medical Group Management Association (MGMA)
The American Medical Association (AMA) and six other organizations have asked two congressional committees to use their oversight of the 21st Century Cures Act to improve interoperability and empower patients with meaningful health information while ensuring data is safe and secure. The letter arrives as the administration is drawing up its plans to implement the law and adopt information blocking rules.
The AMA appreciates several of the administration’s proposals, particularly related to electronic health record (EHR) certification, EHR application programming interfaces (APIs), and modifying EHR vendor business practices and behaviors.
There are, however, numerous complex, counter-intuitive proposals that jeopardize the goals Congress outlined in the Cures Act. Concerningly, many of the administration’s proposals will dramatically affect patient privacy and safety as well as as data security. The proposals also will add to physician burden and burnout.
“The administration owes it to patients, physicians, Congress and our nation to listen and act on these concerns,” said Jesse M. Ehrenfeld, M.D., chair of the AMA’s Board of Trustees. “We still have a chance to get these policies right. It is possible to improve access to medical information while promoting privacy and transparency.”
 More than half of Americans have experienced the sick feeling that comes with opening a medical bill they assumed would be covered by insurance. Surprise medical bills are on the rise, often driven by services administered at an in-network facility using out-of-network providers.
More than half of Americans have experienced the sick feeling that comes with opening a medical bill they assumed would be covered by insurance. Surprise medical bills are on the rise, often driven by services administered at an in-network facility using out-of-network providers.
 Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine
Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine Last month, I was honored to join some of the country’s most elite healthcare executives at the
Last month, I was honored to join some of the country’s most elite healthcare executives at the