As significant changes continue to reshape the U.S. healthcare system, The Physicians Foundation – a nonprofit organization that seeks to advance the work of practicing physicians and help facilitate the delivery of healthcare to patients – has identified five critical areas that will have major impact on practicing physicians and their patients over the next 12 months. The Physicians Watch List for 2015 is based on the Foundation’s insights into the medical practice landscape, supported by data from its 2014 Biennial Physician Survey of 20,000 physicians and other Foundation research and white papers.
Consolidation Hits the Gas Pedal
An increased rate of consolidation among hospitals and health systems continues to drive smaller, independent medical practices into larger systems. This trend is adversely impacting competition in regions where consolidation is most pronounced, while increasing costs and reducing patient choice. Rapid medical consolidation is also presenting a challenge to clinical autonomy. According to the Foundation’s 2014 Biennial Physician Survey, more than two-thirds of all physicians (69 percent) expressed concerns relative to clinical autonomy and their ability to make the best decisions for their patients. Since the rate of medical consolidation shows no signs of abating, it is imperative that hospitals and physicians work together to ensure that clinical decisions are being made independent of any bureaucratic or organizational pressures that could potentially affect the integrity of medical decision-making.
External Pressures Strain the Physician/Patient Relationship
An inadvertent effect of medical consolidation and the rising emphasis on valued-based payment models is increasing strain on the physician / patient relationship. According to the Foundation’s most recent Biennial Survey, 80 percent of physicians describe patient relationships as the most satisfying factor of practicing medicine. Yet, factors such as growing levels of non-clinical paperwork and rising administrative and regulatory pressures are leading to an erosion of quality face-time physicians are able to spend with their patients.
In addition, these pressures can also limit physicians’ choices in terms of practice type while increasing the amount of time and resources they must spend on negotiating with payers and vendors. As these regulatory and marketplace forces persist, it will be more critical than ever for physicians to identify ways to work with support staff in order to maximize the amount of quality time they are able to spend with their patients.
Being adiehard Kennedy fan, this is what I’d normally quote to someone purchasing the latest commodity, or acquiring the latest service that everyone is flocking to stores to get – Conformity is the jailer of freedom and the enemy of growth. However, outsourcing medical billing is a different ballgame altogether.
I’m often confronted by worried physicians who are already overwhelmed by a recent deployment of an electronic health record (EHR) system at their practice when they hear that the clinic next door is outsourcing medical billing. With an expression that could easily pass off as ICD-9 code number 564.0 (a person suffering from constipation), the hesitantly ask me this: “Why is everyone outsourcing medical billing; and even if they are, why should I?”
In response to all those people and all the physicians out there having similar questions, here’s why:
1. It costs significantly lesser
Medical billing companies charge rates as low as three percent of your monthly collections to handle this process for you. Compare this with the costs of a dedicated medical billing department at your practice, and the difference will be significantly lower.
The salaries of the staff won’t be the only cost there, as they’ll need a room or office space to work in, desks and chairs to work on, dedicated equipment (computers, fax machines, printers), and miscellaneous expenses, such as stationary in addition to utility costs. Now when you accumulate all of this with the insurance packages of these staff personnel and the maintenance of this equipment, you’ll realize that the percentage of collections work out a lot cheaper.
2. A large staff base
Each practice assigns a specific budget for billing according to which many small and medium sized practices are able to employ one or two billers who handle all of the practice’s billing related tasks.
More often than not, these understaffed and overworked personnel come across situations whereby they have to decide between negotiating over denied and underpaid claims, or moving on to the numerous pending cases. Given their constraints, they choose to move on, settling for lower (sometimes zero) payments on such claims.
The large staff base of a medical billing company will rid you of this problem as they’ll have different personnel to handle different processes, resulting in the maximization of reimbursements.
Guest post by Tom S. Lee, Ph.D., CEO & Founder, SA Ignite.
If the few years since the onset of meaningful use haven’t been proof enough, the speed and unpredictability of regulatory change in the last five months has cemented our field’s status as truly not-for-the-feint-of-heart.
Yesteryear’s glacial rate of change in healthcare IT regulation is nowhere to be seen. May 2014 brought both a CMS reset of the ICD-10 transition deadline to October 1, 2015, and a proposed meaningful use rule to enable the use of 2011 edition certified EHR technology (CEHRT) to meet compliance in 2014. The summer then ended with the August 29th finalization of the 2014 meaningful use final rule, the ensuing disappointment that the mandated start of Stage 2 was not delayed and then the swift Congressional response in the form of the September 15th proposed Flex-IT Act to introduce quarterly meaningful use reporting for 2015; enough to spin heads more than once around.
What’s happened in the field since the publication of the final rule among provider organizations bring the phrase “threading the needle” to mind. To further illustrate, we have culled some sample issues from our client base of more than 8,000 providers, across more than 15 EHR brands, and representing numerous combinations of meaningful use stage, payment year and program. These issues, none of which yet have universal and clean solutions, span three areas for provider organizations as seen in the field: 1) properly adhering to the requirements of the final rule, 2) working within the constraints of what EHR vendors can deliver per the final rule’s timeline, and 3) redirecting or pausing organizational momentum for change on short notice.
Regarding the first consideration, note that the final rule requires that an organization attest that it is “not able to fully implement” 2014 Edition technology because of “delays in 2014 Edition CEHRT availability.” Although the rule outlines what does not meet this eligibility test, provider organizations have a persistent question about what documentation and conditions are sufficient to satisfy the test.
Guest post by Allison Errickson, CPC-H, director of coding compliance, ProVation Medical, with Wolters Kluwer Health.
Never before have effective revenue cycle management strategies been so critical to future positioning in hospitals and health networks. In today’s lean environment of declining and unpredictable reimbursement, effective oversight of timely billing practices can simply be a make or break element to success.
Because the revenue cycle is dependent on the time-to-bill for procedures and diagnostic care, healthcare organizations must enact processes to support the most efficient coding practices to speed receipt of payment. Success in this area remains an obstacle for many organizations struggling with how to allocate limited resources to ensure the most accurate coding and efficient turn-around.
Denials plague the industry in terms of maintaining consistent cash flow. Inaccurate or incomplete documentation can impact as much as 5 percent of revenues if a healthcare organization is experiencing denial rates of 25 percent or more. Revenue is also negatively impacted when documentation does not support the highest level of acuity, minimizing reimbursement potential.
While accurate documentation remains an ongoing issue, resource allocation to effectively address the issue will likely be further impacted with the introduction of ICD-10. The industry has been granted a reprieve with the recent deadline extension of Oct. 1, 2015, but the reality of the transition will be coming into focus very soon. Coding challenges will be exacerbated as coders will now have 72,000 unique procedure codes to choose from, increasing the complexities associated with specificity and accurately coding to the highest level of reimbursement.
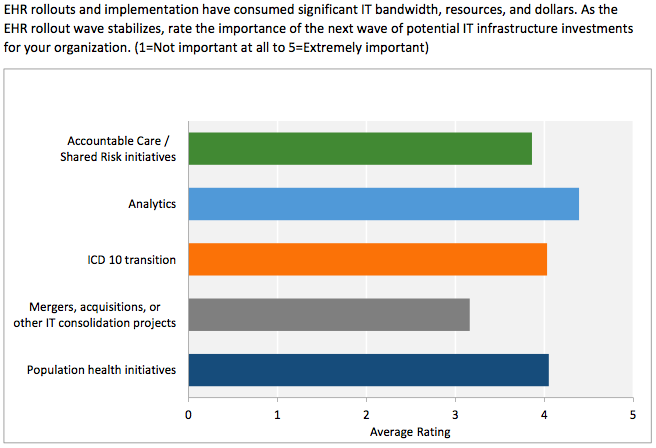
A new survey of senior information technology executives at some of the nation’s largest health systems reveals that their top priority for IT infrastructure investment is analytics – a technology that is central to achieving the systematic quality improvements and cost reductions required by healthcare reform.
Health Catalyst surveyed members of the College of Healthcare Information Management Executives (CHIME), all chief information officers (CIOs) or other senior IT executives of US healthcare organizations. Survey respondents provided a high-level view of the many competing priorities for IT investment that hospital leaders face in the era of “value-based care” – a term describing elements of the Affordable Care Act as well as private industry incentives that reward providers for improving their patients’ health.
Most experts agree that value-based care will require hospitals to use sophisticated analytics to comb through terabytes of clinical and financial data to reveal actionable opportunities for improving quality and efficiency. The survey’s findings confirm that view, with 54 percent of respondents rating analytics as their highest IT priority, followed by investments in population health initiatives (42 percent), ICD-10 (30 percent), accountable care/shared risk initiatives (29 percent), and consolidation-related investments (11 percent).
Lance Speck, general manager of Actian cloud and healthcare, speaks here about healthcare big data and how it can be used in healthcare to improve processes from care coordination to coding for ICD-10. In his day job, he is focused on delivering healthcare solutions to help payers and providers address an estimated $450 billion annual opportunity created through data analytics, ranging from fraud analytics to patient re-admission reduction to staff optimization to accountable care reporting and clinical auto-coding. For more than 20 years, Lance has served in a variety of management, sales and product roles in the software industry including a decade focused on SaaS, cloud and healthcare.
How can big data analytics improve patient care?
According to a recent PwC survey, 95 percent of healthcare CEOs are exploring better ways of using and managing big data; however, only 36 percent have made any headway in getting to grips with big data. All agree that big data analytics has the potential to improve the quality and cost of care, but many are still struggling with finding the right ways to infuse analytics into everyday operations. Assuming they realize that they already have access to the data, what do they do with it? What are the areas that will have the biggest impact? Where do they start?
Start with the basics. Organizations should focus in infusing big data analytics where a big impact can be recognized. They should ask themselves:
Is there enough value in solving the problem?
Can the problem can be predicted?
Can the problem be prevented?
Can the predictive action be delivered accurately, and in a timely fashion to make a difference?
Very early in the process, organizations should address how they plan to incorporate big data into the everyday workflow of clinicians, financial staff and other healthcare stakeholders for organizations to:
Use predictive analytics against historical and external data to anticipate patient occupancy needs to adjust staffing levels to have the right care available at the right time.
Use science to determine with accuracy health trends in specific communities and take action to prevent costly
Determine patients’ risk of readmission before they are discharged to improve patient outcomes and reduce costs and penalties by nearly $70 billion.
Realize that for this insight to be effective, you must put this information into the hands of the clinicians and the patients in the format that fits their daily flow.
How can healthcare providers transition to ICD-10 as simply as possible?
Guest post by Michael Murphy, MD, co-founder and CEO, Scribe America.
In May 2014, the Department of Health and Human Services released findings of their most recent study pertaining to reimbursement amounts provided to outpatient physicians for evaluation and management services. The study uncovered that Medicare overpaid outpatient physicians close to $7 billion and most improper payments were results of errors in coding and insufficient documentation (Table 1, highlights the percentage of claims that were wrongfully claimed for in 2010.). However this is not a problem isolated to physicians from the outpatient clinics, as physicians from inpatient clinics could also be found guilty of miscoding and insufficient documentation.
Recovery audit contractors (RACs) were created by the Medicare Modernization Act to evaluate the accuracy of Medicare claims. If a claim is determined by RAC to be flawed for any one of the many different reasons, the claim is denied. Although Medicare’s retrospective program of auditing bills is good, it is not perfect. There has been a huge spike in appeals of Medicare payment decisions, from hospitals mainly, since the introduction of the auditing program and delays in the appeal process has resulted in hospitals facing great financial difficulties as a lot of their funds are tied up till the appeal has been heard.
Adapted from : “Improper payments for evaluation and management services cost medicare billions in 2010”
In order to receive reimbursement from Medicare, a physician needs to follow a three-step process: 1) appropriate coding of the service provided by utilising current procedural terminology (CPT); 2) appropriate coding of the diagnosis using ICD-9 code; and 3) the Centers for Medicare and Medicaid Services (CMS) determination of the appropriate fee based on the resources-based relative value scale (RBRVS). It is not surprising that physicians often incorrectly code patient visits and procedures as there exists a truly daunting number of codes from which to choose. Moreover, coding structure and reimbursements schemes are constantly evolving and becoming more complex, resulting in a coding process that is often cumbersome and difficult.
Guest post by Keith Boyce, vice president of business development, RxOffice.
The recent postponement of the implementation of ICD-10 is nothing but good news. Moving the deadline to next year gives providers an opportunity to conduct further research and select the software that is compliant and the least disruptive of their existing processes while keeping the best interest of the patient in mind.
ICD-10 was the first step by the Obama administration’s healthcare plan, Obamacare, which revealed the need for a universal software platform that could work in all medical areas. Some professionals say the ICD-10 and other requirements of the new healthcare plan will cause physicians to spend more time on paper work and less time with patient care. If that is the case, healthcare providers will need a system that will cut down on the amount of time needed for paperwork. With the extension in ICD-10’s implementation, now is the time to make decision about keep or modifying current systems or investing in new ones.
The new regulations proposed through Obamacare will have more of an effect on small to mid-size healthcare providers and the IT companies that cater to them. Larger IT firms are not affected as much because their clients are the hospitals and large research clinics that do not have to adhere to the requirements of ICD-10. This means that these firms are less likely to understand and provide compliant software to smaller, special medical centers, such as diabetes, mental health and podiatry to name a few.
Healthcare providers should look for systems with the following characteristics: