Like retail and education before it, a major shift is underway in the healthcare industry that is putting power back in consumers’ hands. Similar to how retail outlets are delivering custom experiences based on consumer preferences, or how there is more attention to individual needs in the classroom, patients are able to play a more active role in their healthcare administration and decision-making than ever before. This means participating in a shared decision-making model with physicians, seeing their needs and preferences reflected in the course of their treatment, and easier access to their medical data, made readily available to both the patient and his or her medical team.
This article will explore the phenomenon that is PCC, a paradigm shift changing the healthcare industry at its core. So much so, PCC is driving adoption of three technology related trends that are in line with its principles. They include: telemedicine, cloud computing and mHealth.
Patient Centered Care and 2016 Healthcare IT Trends
Telehealth
While many assumed in-facility care would remain the norm after house calls faded from popularity decades ago, that may not be the case. Increasingly, telemedicine — or remote consultations, diagnoses, and treatment performed by medical professionals — is becoming a standard practice in the healthcare industry.
For example, the below ad from Anthem BlueCross and LiveHealth Online was released by one of the nation’s largest insurance agencies promoting remote consultations states the “doctor is always in” and sessions are “quick and easy with no appointments and no driving.”
In line with the principles of PCC, telehealth promises greater access to care for patients who don’t live in close proximity to a healthcare facility. For the greater population, telehealth offers convenience and the comfort of care delivered in a patient’s natural environment. Administering care in a patient’s environment instead of a traditional healthcare setting can also facilitate better care in some cases. Fierce Healthcare provides the example of blood pressure screening – taking a patient’s blood pressure in a natural setting, like their home or workplace, may more accurately reflect their blood pressure on a daily basis.
Telehealth and the benefits this practice offers to patients are perfectly in line with the patient-centric approach favored today. In light of this, it wouldn’t be surprising if telemedicine adoption continues to rise in the coming years, along with the demand for technology that can facilitate remote care.
In the age of the digital hospital and the connected patient, security will likely improve the less it depends on providers.
Everything from HIPAA to patient engagement treats physicians as the white hot sun of the healthcare universe, holding everything together and keeping it all in stable orbit. They are accountable for health outcomes, for patient satisfaction, for guiding patients to online portals, and for coordinating with care teams to keep data secure — even as mobility and EHR dominance complicates every node in the connectivity chain. All this digital chaos brings more diminished security.
Only as Strong as the Weakest Link
Every business out there has learned — usually the hard way, or by watching someone else learn the hard way — that whatever the security infrastructure, users are the weakest link. More devices means more users, and more connectivity and data-sharing means more weak spots all along the chain. By design, the EHR system adds vulnerability to healthcare data security through a long chain of users.
Patients don’t have a systemic, accountable role in all of this. Our whole approach fosters passivity on the part of the patient and paternalistic assumptions on the parts of caregivers and policymakers. We give tacit acknowledgement of this imbalance whenever malpractice law or tort reform is mentioned — and promptly left behind in the face of other, patient-exculpatory programs and initiatives.
Patients are a part of this. Clearly they are invested in their own security — the costs of health data breaches contribute to the rising costs of care, besides exposing personal financial and medical information that can carry its own universe of costs.
Patients are implicated, but they must also be accountable for security in the new high tech healthcare system.
An Old Problem with New Importance
Getting patients included in the evolution and delivery of healthcare requires engagement. The same goes for digital security. The ethical and financial dilemmas of the security situation is an expensive distraction for administrators and caregivers, but it is a learning opportunity that could empower patients. A new emphasis on digital security and privacy could be the start of a cascade of engagement with further questions of use and responsibility for outcomes.
Already, patients are key players in making telemedicine effective. Access is on the shoulders of the patients, and utilization depends on their technical literacy. The incentives–time and money savings, improved access to care–are powerful, but come with the obligation to learn the platform through which remote care is delivered. Utilizing any telehealth solutions requires patients to think about what information they want to share, whether they trust the new platform, communicating effectively with their provider, and gaining confidence for the new medium.
This same model can be applied more broadly to EHRs, and the patient role in the digital healthcare system.
Guest post by Ken Perez, VP of healthcare policy, Omnicell, Inc.
Ken Perez
Quality expert W. Edwards Deming was famous for many concepts, including the Deming Wheel or Deming Cycle, more formally known as the PDSA (Plan-Do-Study-Act) Cycle. It is a systematic series of steps for gaining valuable learning and knowledge for the continual improvement of a product or process.
The Centers for Medicare and Medicaid Services’ August 25 release of 2015 quality and financial performance results for Medicare accountable care organizations (ACOs) reflected the application of the PDSA Cycle by the participating organizations as well as CMS in its continued development and refining of its ACO programs.
At a high level, in 2015, the 404 reporting ACOs—392 in the Medicare Shared Savings Program (MSSP) and 12 in the Pioneer ACO Model—achieved $466 million in savings. A bit more than half of the ACOs (210 or 52 percent) held costs below their benchmark, and slightly less than a third (125 or 31 percent) generated savings above a minimum savings rate (MSR) and met quality performance standards, thus meriting shared savings.
As is common with most statistics and especially any material news coming out of Washington, D.C. nowadays, there were widely divergent interpretations of these results.
On the cheery side, CMS chief medical officer Patrick Conway, M.D., rhapsodized, “Accountable Care Organization initiatives in Medicare continue to grow and achieve positive results in providing better care and health outcomes while spending taxpayer dollars more wisely.”
In contrast, Clif Gaus, CEO of the National Association of ACOs, in an email message to FierceHealthcare, struck a negative tone in his appraisal of the results, sharing that his organization “was disappointed not to find stronger financial results that reflect the extensive financial and personal contributions invested by ACOs” and he also said that CMS and Congress must “take swift and decisive action to solidify the foundation of the Medicare ACO program.”
Despite these obviously divergent views, certainly neither Conway nor Gaus would disagree with the idea that the ability to learn is a critical success factor in ACO performance.
A deeper analysis of the data bears this out. As noted by CMS, more-experienced ACOs were more likely to generate savings above their MSR. In performance year 2015, 42 percent of ACOs that started in 2012 generated savings above their MSR. This compares with 37 percent for ACOs starting in 2013, 22 percent for 2014 starters, and 21 percent for 2015 starters.
The value of learning from experience was also reflected in the quality results. MSSP ACOs that reported quality measures in both 2014 and 2015 improved on 84 percent of the measures common to both years.
Guest post by Abhinav Shashank, CEO and c0-founder, Innovaccer.
Abhinav Shashank
Former US President Abraham Lincoln once said, “Give me six hours to chop down a tree and I’ll spend four hours sharpening the ax.” After having a look at the efficiency of the US healthcare system, one cannot help but notice the irony. A country spending $10,345 per person on healthcare shouldn’t be on the last spot of OECD rankings for life expectancy at birth!
A report from Commonwealth Fund points how massive is US healthcare budget. Various US governments have left no stone unturned in becoming the highest spender on healthcare, but have equally managed to see most of its money going down the drain!
Here are some highlights from the report:
The US is third when it comes to public spending on health care. The figure is $4,197 per capita, but it covers only 34 percent of its residents. On the other hand, the UK spends only $2,802 per capita and covers 100 percent of the population.
With $1,074, the US has the second highest private spending on healthcare.
In 2013, US allotted 17.1 percent of its GDP to healthcare, which was highest by any OECD country. In terms of money, this was almost 50 percent more than the country on the second spot.
In the year 2013, the number of practicing physicians in the US was 2.6 per 1000 persons, which is less than the OECD median (3.2).
The infant mortality rate in the US was also higher than other OECD nations.
Sixty-eight percent of the population above 65 in the US is suffering from two or more chronic conditions, which is again the highest among OECD nations.
The major cause of these problems is the lack of knowledge about the population trends. The strategies in place will vibrantly work with the law only if they are designed according to the needs of the people.
What is Population Health Management?
Population health management (PHM) might have been mentioned in ACA (2010), but the meaning of it is lost on many. I feel, the definition of population health, given by Richard J. Gilfillan, president and CEO of Trinity Health, is the most suitable one.
“Population health refers to addressing the health status of a defined population. A population can be defined in many different ways, including demographics, clinical diagnoses, geographic location, etc. Population health management is a clinical discipline that develops, implements and continually refines operational activities that improve the measures of health status for defined populations.”
The true realization of population health management (PHM) is to design a care delivery model that provides quality coordinated care in an efficient manner. Efforts in the right direction are being made, but the tools required for it are much more advanced and most providers lack the resources to own them.
Countless Possibilities
If population health management is in place, technology can be leveraged to find out proactive solutions to acute episodes. Based on past episodes and outcomes, better decision could be made.
The concept of health coaches and care managers can actually be implemented. When a patient is being discharged, care managers can confirm the compliance of the health care plans. They can mitigate the possibility of readmission by keeping up with the needs and appointments of patients. Patients could be reminded about their medications. The linked health coaches could be intimated to further reduce the possibility of readmission.
Guest post by Sivan Agranat, M.D., VP, Medical R&D, medCPU.
Sivan Agranat
The successful implementation of new IT solutions can depend as much on user acceptance as on the technical aspects of implementation. Gaining that user acceptance is largely a matter of ensuring stakeholders are part of the conversation during pre-implementation, followed by fully accounting for and meeting end-user needs during roll-out and beyond. Nobody, especially busy doctors and nurses, appreciates having new technology dropped on them; nor should they. Their input throughout the process is critical not only to their acceptance, but also to solution optimization.
The following is a suggested course of action for gaining stakeholder buy-in and sustained satisfaction that can make new technologies a welcomed addition to clinical care settings.
The technology selection process
Provider organizations invariably have some clinicians who appreciate the benefits of health IT more so than others, and who serve as internal IT champions. When their opinions are respected by their peers, they can be invaluable allies in new implementation projects, which is why it’s imperative to loop them in as clinical representatives at the beginning of the vendor selection process. Their combination of clinical expertise and affinity for IT can be indispensable in validating vendor claims, ensuring the most promising solutions rise to the top. Additionally, having been involved from project start can help enable them to be better positioned to promote the solution internally and offer meaningful support to their peers as they gain user proficiency.
One important element that’s too often overlooked is: When gathering input from clinical representatives during vendor selection, pay close attention to ensure solution capabilities align with existing workflows. Making later adjustments to ensure the right information is delivered to the right person at the right time can be costly and time-consuming.
Before making a final decision on vendor selection, hold an all-stakeholder preview meeting. This can help head off resistance while gaining needed input. Include all targeted end users, not just nurses and doctors, but members of the nursing and clinical support teams as well. If the implementation is a major initiative, consider having meetings with primary stakeholders and include an introduction by the Chief Medical Officer, who can best explain the project’s importance.
In all stakeholder preview meetings, begin by describing how and why the project transpired and what it is designed to accomplish. Next demonstrate the solution and engage people and ask for their feedback. Most importantly, take all feedback to heart, and address stated concerns as clearly as possible. This attention and courtesy can help ward off skepticism at time of rollout, and help ensure acceptance. Also, you may learn from the end user feedback that will help foster enhanced final adjustments before the actual rollout.
Guest post by Valerie Gleaton, managing editor, Health eCareers.
Valerie Gleaton
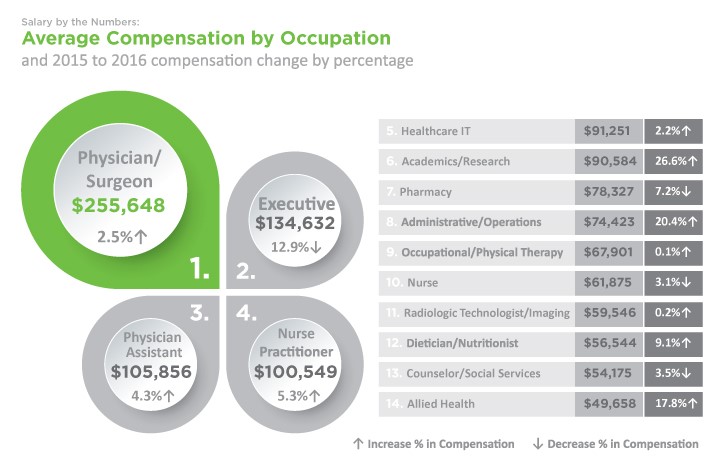
Salaries for healthcare IT professionals are on the rise, but they aren’t growing as fast as some other healthcare positions. That may be impacting satisfaction levels, according to a recent survey. Healthcare job site Health eCareers polled nearly 20,000 U.S. healthcare workers and found that the average annual salary for healthcare IT professionals increased 2.2 percent from 2015 to 2016. However, some of the other positions included in the survey saw more sizeable gains. For instance, those working in academics, research, administration, operations and allied health saw compensation increases in excess of 10 percent.
With more available jobs than professionals to fill them, hospitals, healthcare clinics and other providers are increasingly willing to loosen their purse strings and pay higher wages to both current employees and new hires. These factors have created a perfect storm of opportunity for healthcare workers, and 87 percent report that their pay is the same or has increased compared to a year ago. Survey respondents pointed to merit raises or employer changes as the primary reasons for their increase. There were exceptions, however. Nurses and healthcare executives saw a 3 percent and 13 percent drop, respectively.
$91k is Average for Healthcare IT
Healthcare information technology professionals are enjoying robust job prospects, as healthcare organizations come under the gun to improve efficiencies, cut costs and find better ways share patient information. The study revealed that America’s healthcare IT workers earn an average of $91,251 a year, the fifth-highest paid healthcare profession, topped only by physicians/surgeons, healthcare executives, physician assistants and nurse practitioners.
Pay Fluctuates by Location, Experience and Position
Location seems to influence pay, with salaries varying widely from state to state. For instance, healthcare IT professionals in California earn an average of $95,224 per year, while their counterparts in Texas make nearly 6 percent less, averaging $89,758 a year.
Another large and unsurprising determinant of pay is experience. New healthcare IT professionals — those with five or fewer years of experience — earn an average of $74,815 per year, while those with more than 10 years of experience report an average annual salary of $104,343. Those that fall in the middle with 6–10 years of experience pull in an average of $98,082.
Health eCareers also found big pay discrepancies by types of healthcare IT disciplines. Health information technology executives are far and away the best paid, with a median annual income of $127,500. IT technology managers also do well, with median earnings of $111,500 per year. Further down the pay scale are healthcare informatics employees at $74,500, and toward the bottom are health information technicians, who report median salaries of just $50,500.
Guest post by Lea Chatham, editor-in-chief, Getting Paid, a Kareo Resource.
Lea Chatham
Patient engagement has been the hot topic of this past year or two. Everyone agrees that engaging patients more in their healthcare can help reduce costs and improve overall health. A study conducted by HIMSS in 2015 showed that the majority of physicians believe patient engagement is beneficial and should be a part of their job. However, the study also concluded that over 40 percent of physicians worry that there is little reimbursement for engagement activities.
Patient are looking for more ways to connect with providers from online scheduling to text reminder to email follow ups and social media. And while many see these as conveniences, the reality is that they do also improve health and have the potential to reduce costs. Studies have shown that simple follow up communications via text and email can help ensure patients show up for appointments and can reduce hospital re-admissions, which has a big impact on healthcare costs.
Unfortunately, physicians are already stretched thin trying to care for patients, run their practices, adhere to complex programs like meaningful use and PQRS, and navigate changes like ICD-10. Who has the time to do more? And many providers worry that “engagement” means more work with less reimbursement. But it doesn’t have to be that way.
In fact there are many opportunities to automate engagement and provide the tools patients want without adding any time or effort to a provider’s plate. Today, there are solutions that once set up enable easy online scheduling, text and email reminders, follow up patient surveys, and even re-care programs.
This infographic highlights some of the feelings of both patients and providers feel about patient engagement and shows how practices can utilize engagement strategies that benefits both and do have a financial return.
The huge growth of the home care industry in recent years has led to a Catch 22 situation. On the one hand, people are living for longer than ever before and the number of home health aides is growing at a rate far higher than the average for all industries. On the other, the increase in life expectancy means that the number of elderly people requiring home care has never been higher, and even the increase in home care workers isn’t enough to cope with demand. Also, the tightening of licensing regulations will shrink the pool of available caregivers.
In this infographic from Be Independent Home Care, we can see that the home care industry is at a crossroads and faces into a potentially troublesome future. By 2024, the number of home health aides is projected to have grown by 38 percent from a decade previously. By 2020, the global homecare industry is expected to produce revenues of $300 billion, compared to $180 billion in 2014. All the while, the senior citizen population in the U.S. has doubled from just four years ago, with one in five Americans now of senior age.
Where does the home care industry go from here? Quite simply, it needs to keep adding to the number of qualified caregivers – just at an even faster rate than at present. That won’t be easy considering that the current rate is well above the overall average, but unless that rate is maintained, demand will exceed supply and then there really will be a home care crisis. Here, perhaps, is the epitome of being a victim of one’s success.