Nurses play an all important role in healthcare’s shift from sick care to wellness-based models as the front-line professionals closest to patients. Always an intricate balance of art and science, nursing practice most continue to evolve to place patients where they should have been all along—in the center of care.
An independent survey commissioned by Wolters Kluwer of nearly 2,000 consumers, nurses, doctors, and healthcare executives in the U.S. provides insights into the top trends that will shape priorities over the next few years – for care teams, hospital leaders, health systems and consumers.
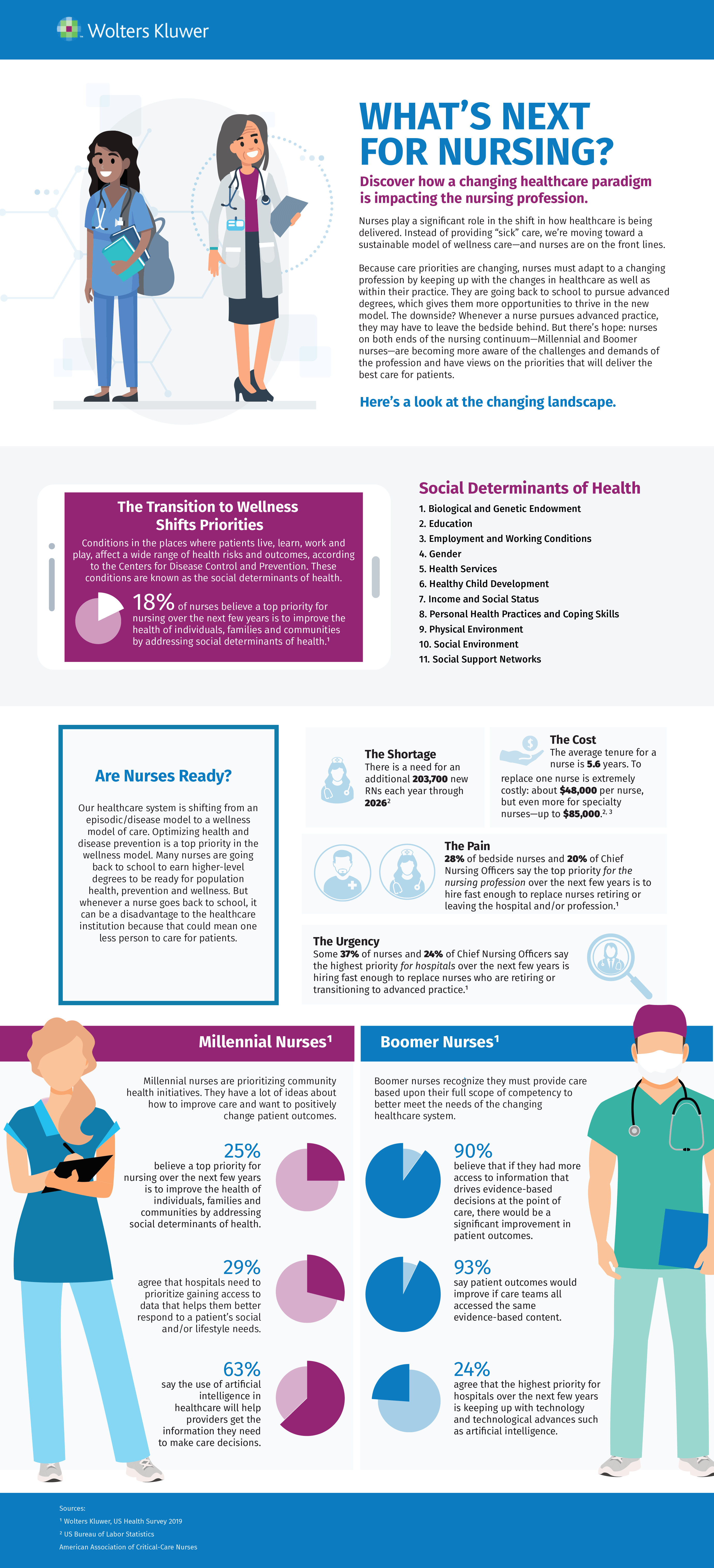
The below infographic details key findings related to challenges and opportunities impacting the nursing profession including perspectives on:
the impact of professional shortages
the growing importance of holistic care that addresses social determinants of health
generational differences between practicing nurses
More than ever, nurses need to demonstrate knowledge, confidence, competence, professionalism, empathy and kindness. And they need to be equipped with the right evidence-based tools and education resources to thrive in a changing healthcare landscape.
Addressing the social determinants of health (SDoH) in communities is a hot topic of conversation in healthcare. The industry has bought into the theory that 20 percent of an individual’s health is determined by clinical care and the rest by social, economic, genetic and behavioral factors. But perhaps more importantly health systems need to recognize that they can’t solve this issue on their own.
From my perspective at PCCI, I’ve seen an increase in value-based contracting models in recent years, and health systems and physicians are looking beyond the four walls of their institutions to build relationships with outpatient, behavioral health, post-acute care, and now non-medical providers. The number and types of collaboratives between health systems and non-traditional providers has been growing over the past several years with a recent report gathering information on more than 200 different partnerships between hospital and community-based organizations across the country.
But while health systems may be embracing community provider relationships, I believe that sustainable success in addressing social determinants of health requires a fundamental shift in the way health systems view their role in improving the health of their communities.
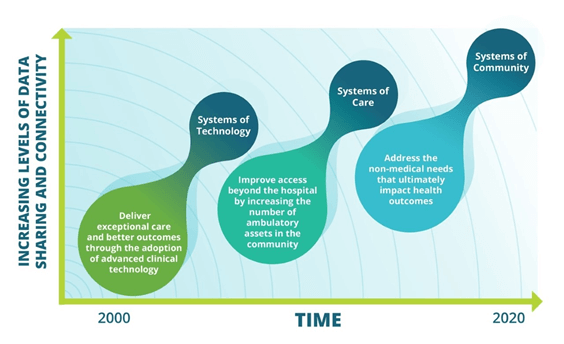
Over the past ten to fifteen years there has been an evolution in how health systems have approached improving health outcomes. Initially health systems focused on providing high-tech solutions for care delivery such as robotic surgery, and advanced imaging techniques. Then to meet the need for increased access and demand for outpatient services, health systems seeded service areas with ambulatory surgery centers, urgent care, retail clinics, and physician offices.
In each of these evolutions the strategies centered on a solution created by the health system alone. And one could argue that the main beneficiaries of these investments were often the health systems themselves – increased market share, improved reimbursements. But such a self-centered approach will not work when addressing social determinants where the root causes lie outside the four walls of the health system.
Effectively creating a system of community will require a collaborative mentality from health systems. While they may have power and influence to gather partners to the table, execution of successful interventions lies with social services and community-based organizations that are the experts in understanding and helping individuals address social needs. Even if not leading, health systems should still be active participants in this work. Indeed, there are areas where their contributions to the organization of partners is critical:
Carrot Health, a provider of healthcare solutions powered by social determinants of health (SDoH), announced it has been named a finalist in the Accenture HealthTech Innovation Challenge – Health North America. Carrot Health was one of 13 companies to compete in the Boston regional round of the competition, which supports innovative technologies and drives creative solutions to improve the way people access and manage healthcare.
“We are honored to have advanced to the finals in this important program. Innovation is the engine that drives crucial improvements in healthcare, such as the ability to leverage key SDoH data to close critical care gaps by addressing the non-clinical needs that impact as much as 80% of health outcomes,” said Kurt Waltenbaugh, CEO of Carrot Health. “The caliber of technology solutions presented by our fellow competitors in the Boston round of the HealthTech Innovation Challenge was outstanding, and we are honored to have been among them.”
Carrot Health, which moves on to the finals taking place in Houston in February 2020, was selected for its Carrot MarketView platform, which generates insights for growth, quality and health using social, economic, behavioral and environmental data. MarketView helps healthcare organizations by leveraging consumer and clinical data to deliver a 360-degree view of the patient.
Validated in the market, Carrot Health’s predictive models and insights have proven effective at:
Driving growth by identifying consumer needs
Improving health outcomes by influencing key performance metrics, such as emergency department utilization, admission/readmission, cost of care and mortality
Enhancing quality by closing care gaps and improving customer satisfaction
“MarketView encourages health organizations to address appropriate needs along the full healthcare hierarchy, identifying and eliminating bottlenecks before they can adversely impact quality, care outcomes and costs,” said Waltenbaugh.
Since its inception, the Accenture HealthTech Innovation Challenge has brought healthcare organizations and startups together to tackle the world’s biggest health issues. Over the life of the program, Accenture has received more than 2,200 applications, invited more than 90 startups to compete, benefitted from the time and guidance of nearly 1,000 executive judges, and awarded 10 trophies to the most innovative healthcare startups. The Health North America challenge brought together innovative startups across North America to compete in a challenge focused on solutions in the areas of operational efficiency, increased access and consumer experience.
The term “social determinants of health” is far more than a trendy new buzzword in health care. Serving the physical, mental and social needs of the community is not just the right thing to do but can mean substantial improvement in care and reduction in unnecessary healthcare costs.
Several studies have shown that addressing social needs, such as food or housing insecurity, can have a significant impact on a person’s healthcare outcomes and costs. Individuals experiencing housing insecurity or homelessness have higher rates of chronic diseases such as high blood pressure, heart disease, diabetes, asthma, chronic bronchitis, and HIV. This in turn leads to higher utilization of healthcare services such as emergency room visits, inpatient hospitalization and longer lengths of stay compared to those individuals with secure housing. Similar results are seen in those experiencing food insecurity.
Hospitals often state that part of their mission is to provide high quality care and improve the community’s health, or community benefit. A recent study of hospital mission statements in three states (Ohio, Florida and Texas) found that while quality was cited most often (65%), the second most frequently used term was community benefit (24%).[1] If community benefit or community health is part of your health system’s mission statement, how much are you really doing to address the whole health of a community vs. just addressing their “sickness” needs?
At PCCI, our combination of data scientists and expert clinicians believe that health systems have an obligation to address social determinants of health to ultimately remove the disparities and inequality that we see in our community’s health. Yet this is tricky because success requires outreach skills, community relationships and data insights that extend beyond the traditional promise of health-related services. That said, there are three key elements that can assist health systems in making an investment in social determinants of health a reality. To move from theory to action, my suggestion is that health systems do the following:
Leverage the board’s community presence to align on areas of greatest need
As part of health system leadership, board members ensure alignment between mission and a defined SDoH strategy at all levels of the organization. As community representatives themselves, board members can also create the momentum and connections that health systems need to bring community and business partners together to create a governance structure for launching a connected community of care. Such governance structure will guide the strategy, legal and policy needs, and the investment and execution of a connected and aligned SDoH strategy.
Invest in long-term partnerships to ensure sustainability
Recognize that as health systems, you alone cannot solve for social determinants. To truly meet the social, behavioral and emotional needs of some of the most vulnerable individuals in your community, you need to identify community partners with expertise in these areas. With the assistance of board members, assemble a partnership collaborative, with a formal governance structure, to build community-based strategies around SDoH needs. Support the sustainability of this collaborative with technology and data science techniques to identify specific root causes of social need in target populations, share data, and measure impact of interventions. Identify an independent partner to evaluate the effectively of the SDoH initiatives and measure the cost, savings and impact across the community and for the health system.
What is that one factor that separates one patient from another? Can one identify why two patients with the same illness but from different regions respond differently to a particular treatment? Do we need to cater to the needs of patients even after they leave the clinic?
These questions have always intrigued not only the physicians but every member who is involved in the care journey— care teams, communities, social workers, even patients themselves. And the answer lies in just one fact— even if these two patients appeared similar on paper, their lifestyles are very likely to differ: socioeconomic status, gender, race, ethnicity, family structure, and education.
All of this comes down to just one term: Social Determinants of Health.
This is one of the prime problems that has kept healthcare organizations in a situation of dilemma.
We are way past the statement that SDoH is just another hype
Have you ever tried to score a home run with one hand tied behind your back? This situation is similar to the condition of healthcare organizations in the value-based ecosystem. They are trying to get 100% of the task of healing a patient done with just 50% of the insights.
Social determinants matter because they can affect the health of the population residing in a particular region, for better or for worse. We have countless studies that show the importance of social determinants, yet we are not able to properly address them because we are not able to answer these questions:
How do we address the challenges that we don’t even know exist?
Who is responsible for addressing these challenges?
Is there any ideal strategy to address SDoH?
No matter how famous they are in healthcare, working with SDoH requires a drilled-down approach and something that we have in abundance- healthcare data. This data can be leveraged, and with the use of predictive analytics, organizations can accurately measure the at-risk population and advance preventive care methods in the ecosystem.
The best way, I think, is to look at this picture with a magnifying glass. Traditionally, the endpoint is the state-level analysis of SDoH. However, it is not the end but the beginning of the study that should go to the zip code level.
Here are some of the most interesting stories of how the leaders in the field of addressing the Social Determinants of Health addressed the populations’ needs and did the undoable.
What was the Humana way to deal with the non-clinical factors?
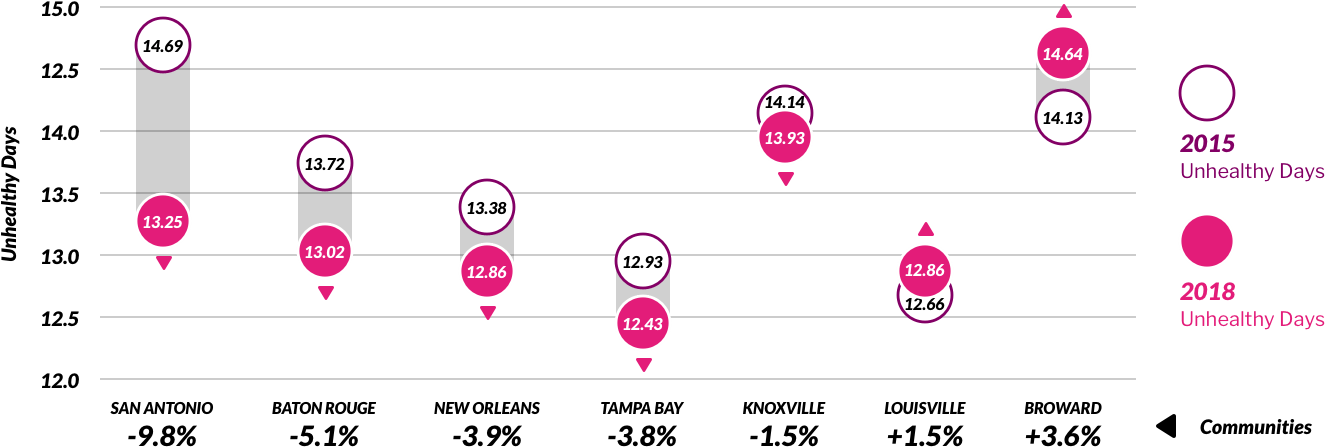
Humana has the Bold Goal Initiative, which is a population health strategy that is aimed at improving the health of the communities and making them 20% healthier by the year 2020. Their Healthy Days surveillance process is a robust and scalable metric. Based on this, they found that food insecurity and loneliness were among the top contributors to the total unhealthy days among the population they serve.
With their holistic and comprehensive approach, they built an analytic intervention pipeline to address these issues. One instance is their intervention with Papa Inc., where they connected college kids to seniors who needed companionship. As a result, 94% of members stated that the Papa Program helped them to feel more socially connected.
Humana was able to reduce the number of unhealthy days from 2015 to 2018 by simply addressing the non-clinical aspects of care delivery for their population.
Performance of Humana’s seven original Bold Goal communities (2015-2018) – Humana Medicare Advantage members
How MercyOne PHSO took the understanding of non-clinical factors from the zip code level to an individual patient level?
MercyOne PHSO, one of the largest ACOs in the Midwest, wanted to know the factors affecting their patients. They took the simple concept of asking the right questions and leveraged it to understand their patients.
While their patients entered the hospital or examination room, they asked them to complete a survey consisting of questions that depict the factors that affect their patients’ health, such as:
In the last 12 months, were you worried that your food would run out before you got money to buy more?
What is your living conditions today?
Do you face any difficulty in reaching out to your doctor?
At this point, most of us in healthcare have read similar statistics about why we need to do more to address social determinants of health (SDoH) — the conditions in which people are born, grow, live, work and age, and how those factors impact individuals’ health — to improve patient outcomes. These conditions and their resulting social needs include, but are not limited to, a person’s equitable access to nutrition, housing, transportation, education, and employment opportunities.
Time is of the essence to tackle some of these social determinants, especially when coupled with the rapidly shifting patient demographic, sometimes called the “silver tsunami.”
Payer
SDoH studies in no short supply
It seems everyone is in a race to figure out what SDoH approach will move the needle toward lower risk for their patient populations. But payers, in particular, have taken on a hefty amount of the leg work needed with social determinant “barriers to care” studies, because they are generally the most financially accountable, from a population health analytics perspective, to remove them.
Recent news about of these payer SDoH pilot programs and research studies have been both interesting and useful across the care continuum, a summary of which include:
WellCare, which provides managed care plans for over 4.4 million Americans, ran a pilot program on over 33,000 patients, referring them to more than 100,000 community-based social services programs, and was able to reduce inpatient spending by 53%, outpatient spending by 23%, and emergency spending by 26%.
In its Bold Goal 2019 Progress Report, Humana focused on patients in specific lines of business, including their Medicare Advantage program, where 91% of seniors who have at least one chronic condition. They enacted the Centers for Disease Control and Prevention’s “Healthy Days” self-reporting method of measuring healthy vs. unhealthy days and have also screened half a million people for SDoH since 2018, with the goal to screen one million by 2019. Humana notes that these social barriers are “deeply personal,” which requires closer partnership to track and measure population health.
Blue Cross is already instituting food, nutrition, and housing services as part of some of its plans. But it also recently announced an investment of $40 million with Solera Health, to address both mental health and SDoH matters, including “food insecurity, medically tailored meals, transportation, falls prevention, and social isolation” with lifestyle modification programs such as diabetes or management, and tobacco cessation programs.
A study by the Anthem Public Policy Institute says individuals and the public (researchers and journalists) perceive SDoH differently. Individuals tend to lead with concerns about the health care “system,” whether they can find the right provider, followed by whether they have adequate “social support.” The public tends to “frame health outcomes through the lens of structural factors like education and income level perhaps, in part, because these factors are easier to measure.”
UnitedHealthcare and the American Medical Association partnered to expand the existing ICD-10 diagnostic codes being used to identify social and economic barriers to care. This adds 23 more codes to that list, some of which would “indicate a patient’s inability to pay for prescriptions, inadequate social interaction, or fears about losing housing.”
Existing
workflows provide best locale for SDoH communication
Despite all of the various innovative steps being taken to bring SDoH to the forefront, we know that most patients still aren’t talking about SDoH concerns with their physicians. There are many reasons why, but one logical solution to bolster SDoH communication between physicians and patients is to incorporate, at minimum, the ability to identify social needs where they are already doing business — in these EHR, CRM, and other third-party platforms.
As is evidenced by the silo’d health IT data systems that have for too long crippled the health care industry’s transparency and ROI, we know that simply identifying social barriers to care is not enough. Within the designated “source of truth” that is most responsible for driving patient engagement, whether that is an EHR, CRM, or other platform, we need to build — or integrate — expanded capabilities for SDoH identification, referrals, and tracking each throughout the continuum of care to close the gaps that currently exist.
That is not to say that physicians must now wear yet another hat — that of a social worker or a social services case manager. But being asked to solve SDoH from the current physician’s workflow perspective, without integrating SDoH into the patient record, is basically saying to physicians:
“Improve clinical outcomes. But first, you must identify non-clinical data, be responsible for referrals to improve these individual circumstances, and track each of those referrals’ progress, all in different platforms, and none of which talk to one another.”
This is not setting our patients or their physicians up for success.
The idea of a standardized SDoH screening mechanism within the EHR has been endorsed by the National Academy of Medicine, the Medicare Access and Children’s Health Information Program Reauthorization Act of 2015, the 2016 Centers for Medicare and Medicaid Services’ Quality Strategy, and several other organizations, as released in an Annals of Family Medicine study. But unfortunately, in this first U.S. study of its kind to address feasibility, “little is (currently) known about how to capture and present (SDoH) information in community health centers’ EHRs.” Nor did the study conclude how to integrate EHR-based documentation needs into community health centers’ existing workflows.
The main barriers cited in the Annals’ study were that EHR-based SDoH tools: (1) Create a too-fragmented view of the patient, with relevant data in too many disparate locations (2) Might add a layer of difficulty to obtain and act on SDoH data (3) If SDoH patient information has been acquired on paper, that requires yet another dual, manual data entry problem when “referral workflows were (already) seen as too time-consuming, especially when no follow-up was planned,” resulting in “an unmanageable follow-up workload.”
To date, the EHR has done a good job of serving most of the goals to take our country’s health records digital. But it is also safe to say that the EHR, in and of itself, cannot be all things to all persons working in health care. In addition to the major enterprise EHR systems, there is a proliferation of specialty, industry-specific EHRs, which may or may not have separate CRM platforms, not to mention all of the other third-party, various other platforms you can see within any one given practice, such as separate billing and referral management types of platforms. There is a reason that “interoperability” among all of these disparate health care data systems has become another hot topic for the industry.
To yield maximum value for our customers, integrating SDoH data is best-approached from a workflows perspective — not just connecting disparate data systems for the sake of “more data,” but to make caregivers’ lives easier, and to create actionable data that enable better business decisions. And we already know that one of the easiest ways to improve efficiency for health care organizations is to remove dual, manual entry between EHR, CRM, and other third-party platforms that hold patient data — these are the first and most valid case studies of how to improve organizational efficiency while bolstering patient care.
There has been a flurry of innovative partnerships and technological improvements to address SDoH, all of which should ultimately be supported by policy changes — each of these as prevailing themes at trade shows and conferences in recent years, such as the America’s Health Insurance Plans’ (AHIP) annual conference, held recently in Nashville. Meanwhile, we look forward to participating in more discussions about how those of us in health IT can do our part — bridging SDoH informational and communication gaps between physicians and patients. This could include integrating non-clinical SDoH concerns into the patient’s clinical record, in and out of these platforms, establishing standards for capturing SDoH to make data-sharing easier, and even incorporating social services databases for more streamlined SDoH-specific “referral management.”
We talk a lot about how to achieve interoperability in healthcare, with all of its disparate data systems, and SDoH is another compelling and recent reason why we must accelerate these solutions, which would ultimately benefit health care and all of its stakeholders — patients, physicians, payers, and everyone in between.
By Hants Williams, director of clinical operations, VirtualHealth.
Hants Williams (Photo by Marcela Nowak)
The buzz around social determinants of health (SDoH) is making waves across the healthcare industry. Linked to roughly 80 percent of overall health, stakeholders are increasingly embracing the opportunity of addressing SDoH in care management workflows.
SDoH are defined by Healthy People 2020 as the “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning and quality-of-life outcomes and risks.” Essentially, these elements encompass the non-clinical factors that can promote or hinder a patient’s ability to fully comply with care plans.
Transportation sits at the heart of current SDoH initiatives as a fundamental prerequisite to optimal care. Simply put, if patients cannot pick up their medications or get to appointments, a provider’s ability to impact their patient’s health is minimized. Consider, for example, a recent Connance survey that links 50 percent of re-admissions to factors such as transportation and home instability risk.
In the era of value-based care, the simple act of helping patients access transportation can notably improve the outlook on clinical outcomes and costs. For instance, medication adherence is a focal point of industry efforts to improve clinical outcomes, but if a patient cannot access transportation to pick up needed drugs, the potential for improvement is minimized.
Access to transportation is low-hanging fruit in terms of performance improvement, and providers must get ahead of the transportation challenge to implement successful, sustainable population health strategies. It’s also why forward-looking organizations are addressing this critical element of SDoH by equipping care managers with tools that speed identification of transportation needs and available services.
Understanding the Challenge; Recognizing the Opportunity
Industry statistics reveal that the transportation challenge is significant and is expected to compound in the coming years. Estimates point to 3.6 million Americans missing or delaying medical care because of an inability to get to their appointments.
Understandably, the transportation issue is exacerbated in low-income and elderly populations as well as rural regions where public transportation is scarce. Many patients simply lack the disposable income needed to maintain a reliable source of transportation. In terms of elderly populations or those with disabilities, physical or mental conditions that eliminate or significantly restrict driving as an option create additional challenges.
The current and coming transportation challenge is sizeable and will require significant resources. Fortunately, the business case for improving the outlook is an easy one to make: A recent study examining non-emergency transportation costs in Florida found that if a mere 1 percent of medical trips resulted in the avoidance of an emergency room visit, the state could save up to $11 for each dollar spent.
Advancing Transportation Strategies
Providers and payers alike are increasingly turning to tools that help identify SDoH needs like transportation in near real-time, allowing care managers to proactively seek out community resources that can help. For example, one state-run managed Medicaid program deployed a care management platform that allows clinical teams to access pre-approved community services and schedule transportation appointments immediately once needs are identified.
With the help of customized algorithms and advanced artificial intelligence tools, drivers can be deployed to patients’ homes in anticipation of needs rather than finding out after the fact that appointments were missed, or medications were not picked up. The efficiency of the analytics platform is critical to changing the dynamic as clinical teams would otherwise be tasked with combing through millions of line items in patient records to identify potential needs.
Advanced solutions allow users to easily monitor transportation requests across all patients or drill down into a single case to manage unique details of each trip, such as advanced authorizations or ensuring the appropriate vehicle has been scheduled to accommodate assistive devices, child seats and companions. Care managers improve efficiency by scheduling recurring trips and tracking specific patient requests or preferences, which can be shared with the transportation vendor and other care coordinators.
Leveraging the transportation functionality, the state-run Medicaid program completed nearly 24,000 transportation entries in 2018. Through advanced analysis, it was able to forecast usage trends across months, time of day and geography to help its clients optimize operations and predict transportation expenditures. For example, the organization can determine which patients are frequent transportation users, which can alert care managers to book multiple provider appointments at once to reduce costs versus on separate days.
Personalized care management and coordination is part of the healthcare industry’s overarching goal of cultivating healthier communities. SDoH indicators such as transportation are critical to these efforts. Forward-thinking organizations are taking hold of the opportunity to improve care management by investing in infrastructures that support greater access to transportation.
By Dr. Chris Hobson, chief medical officer, Orion Health.
Dr. Chris Hobson
Health information exchanges (HIE) help care teams provide more informed patient care by supplying a complete longitudinal healthcare history of the patient to healthcare professionals, as well as enabling high quality reporting and analytics on the data. The goal of an HIE is to accurately store all relevant patient information from as many sources as possible, including medical history, medication history, past treatments and detailed personal information. A comprehensive reporting system allows for health delivery that is more responsive and tailored to each patient, and subsequently, the broader population.
Today the transition to value-based funding models seeks to lower costs and improve patient care and outcomes in order to lead to the better management of entire populations. Population health management (PHM) involves changing the behavior of engaged consumers to lead healthier lives and encouraging physicians to focus on providing the best possible quality of patient care at the lowest possible price. This requires providers to collaboratively address whole populations and orchestrate healthcare provision at large scale. Below are several challenges organizations must overcome before closing in on the goal of PHM.
Payer-provider collaboration and targeted incentives
Payers and providers must work together and, in particular, must find ways to effectively share their different types of data. Collaboration is needed to achieve shared goals such as understanding and improving the health of a population and enhancing the patient experience, all while constraining costs.
A key issue between payers and providers is agreement on the quality measures that will be incentivized. PHM places an unfair, high burden on providers if required quality measures vary widely across payers or if the measure does not clearly reflect a meaningful quality of care indicator. In the latter situation, a provider’s time and effort are used for inefficient purposes adding to a physician’s frustration with the healthcare system. Conversely, payers have additional data that can often help providers significantly with their population health management needs.
Care coordination
Fragmentation of care poses a challenge for health systems globally, and there is research to suggest that this problem is more persistent in the U.S. than its international peer countries. Studies have highlighted the major consequences of a poorly coordinated health system, including delays in care, incorrect care, and unnecessary complications, tests and procedures. Frequently, poor communication, difficulty sharing care plans and challenges coordinating actions by multiple caregivers across organizations results in confusion, delays in care and even incorrect care actions, putting the patient’s health on the line. A health system that is not well coordinated cannot deliver high quality care at lower costs.
Physician involvement in preventive care and the social determinants of health
For physicians, finding ways to move care from the acute setting toward health promotion, disease prevention and addressing the social determinants of health is quite difficult and not something they are necessarily empowered to do today. Currently, the majority of physicians do not have the tools to solve major intractable social issues such as poverty, so involving physicians and patients in the strategic design of a social determinants of health program is an essential step toward resolution of these types of concerns.

 “We are honored to have advanced to the finals in this important program. Innovation is the engine that drives crucial improvements in healthcare, such as the ability to leverage key SDoH data to close critical care gaps by addressing the non-clinical needs that impact as much as 80% of health outcomes,” said Kurt Waltenbaugh, CEO of Carrot Health. “The caliber of technology solutions presented by our fellow competitors in the Boston round of the HealthTech Innovation Challenge was outstanding, and we are honored to have been among them.”
“We are honored to have advanced to the finals in this important program. Innovation is the engine that drives crucial improvements in healthcare, such as the ability to leverage key SDoH data to close critical care gaps by addressing the non-clinical needs that impact as much as 80% of health outcomes,” said Kurt Waltenbaugh, CEO of Carrot Health. “The caliber of technology solutions presented by our fellow competitors in the Boston round of the HealthTech Innovation Challenge was outstanding, and we are honored to have been among them.”
 Is there any ideal strategy to address SDoH?
Is there any ideal strategy to address SDoH?