(Connected Communities of Care Definition: An innovative method for effective population health management using social determinants of health. A way to streamline effective coordination between medical, government and community-based organizations.)
We ask this type of question every day. For example, we may ask? “Is this product that I purchased making a difference?” or “Is this advanced training that I completed making a difference?” Implicit in this common question is the expectation that because we have made an investment in something to achieve a result, the result should be better or more improved than the pre-investment state. So too with a Connected Community of Care (CCC).
As I have discussed in previous blogs, establishing a CCC requires a substantial investment in both time and money. Therefore, it is only natural to ask? “Is this CCC making a difference, and how would I know?” Unfortunately, most CCCs are established with very little forethought given to this exact question. While we expect the CCC will help community residents improve their health and well-being, how will we know conclusively that this has happened?
How will we demonstrate its impact to a potential partner or? more importantly? a funder? This is where data, measurement, and evaluation come into play. For most people, these three words cause anxiety levels to immediately rise. But this doesn’t need to be the case; a little planning and forethought can go a long way to assuaging one’ anxiety when asked the question, “Is your CCC making a difference?”
Before we think about what data we will need to answer this question or how we will collect it, we first need to establish what we mean by “making a difference”. Understand, there is no one correct answer to this question. What may constitute a positive difference or impact for one organization may be much different for another, even similar organization. Many factors contribute to the final answer and each are usually organization-, ecosystem- and situation-specific.
In practice, there are many ways to define making a difference. First, we can look at quantitative or numeric information to make this determination. Are we providing more nutritious meals to indigent residents? Is the number of inappropriate Emergency Department visits declining or, conversely, is the number of residents having visits with a primary care provider increasing? All of these effects can be counted and judged against some predefined goal (more on this later).
Second, we can assess making a difference by asking the people that are being touched by the CCC. Through surveys or brief interviews, community residents can tell you in their own words what impact, if any, the CCC has on their lives. While this qualitative (non-numeric) information can often be more informative than simple quantitative information because it represents the voice of the individual, to answer the question of whether your CCC is making a difference, you will also still likely need to establish numeric goals.
A third way to assess whether your CCC is making a difference is indirectly via the financial and non-financial opportunities that arise as a result of having a CCC versus not having one. For example, having a CCC may make it much easier to perform contact tracing among vulnerable populations during a pandemic like COVID-19. Having a CCC may also enable a healthcare system or a community-based organization (CBO) to apply for a grant that it otherwise might not be competitively positioned to do if it did not have an integrated system of healthcare and social service providers such as a CCC.
We’ve all experienced crises in our lives. They may be personal in nature (e.g., involving our interpersonal relationships), organizational (e.g., relating to our employment or retirement income) or nature-made (e.g., floods, tornados, or the COVID-19 pandemic). When crises hit our communities, the impacts can be widespread and far-reaching.
Healthcare providers and community-based organizations (CBOs) are called upon to provide more rapid and extensive care and support to the community than is otherwise the norm. A well-established and highly functioning Connected Community of Care (CCC), as is the case here in Dallas, Texas, can provide a tremendous strategic and tactical advantage over non-connected peers.
Since 2014, the Parkland Center for Clinical Innovation (PCCI) has led an effort to bring together several large healthcare systems and a number of regional social-service organizations such as food banks, homeless assistance associations, and transportation service vendors, along with over 100 smaller CBOs (i.e., neighborhood food pantries, crisis centers, utility assistance centers) and area faith-based organizations to form the Dallas CCC.
Over time, civic organizations, such as the Community Council of Greater Dallas, Dallas County Health and Human Services (DCHHS), and select academic institutions have begun to participate in various community-wide projects under the Dallas CCC umbrella. Central to the success of the Dallas CCC are the partnerships that have been formed between the CBOs and a number of local healthcare systems (Parkland Health & Hospital System [Parkland], Baylor Scott & White Health, Children’s Medical Center, Methodist Health System, and Metrocare Services), clinical practices, and other ancillary healthcare providers serving the Dallas metroplex. These partnerships have proved essential in building a truly comprehensive and functional network aimed at improving both the health and well-being of Dallas residents.
Connecting these various entities and forming a two-way communication pathway is an electronic information exchange platform termed Pieces Connect, which allows for real-time, two-way sharing of information pertaining to an individual’s social and healthcare needs, history, and preferences.
The information exchange platform is the glue that holds the physical network together and provides one of the mechanisms to disseminate information from public health and healthcare entities to social service providers in the community. It allows the individual community resident, via the CBO, to become better informed about important health issues, such as routine vaccinations or preventive care, such as social distancing and proper mask usage during a pandemic.
Until recently, the primary mission of the Dallas CCC focused on addressing residents’ social determinants of health (SDOH) issues through providing community resources (e.g., food assistance, housing, transportation) to improve the lives of Dallas County residents. While this mission has become even more critical during the COVID-19 pandemic, the work of the Dallas CCC has also evolved to include identifying COVID-19 sites within the County and directing community outreach efforts to help stem the rapid spread of the virus.
This question initially brings to mind many possibilities such as connection to the latest 5G cellular service, a new super-fast internet provider, or maybe one of the many new energy suppliers jockeying for market share from traditional utility companies.
While all of these might represent legitimate opportunities to improve one’s community, here we are talking about a different concept; specifically, whether your community is ready to have a Connected Community of Care (CCC) to advance whole person health.
The image of a CCC may seem obvious. After all, we all live in communities where we have some connections between hospitals, physician practices, ambulatory care centers, and pharmacies to name just a few. But here we are talking about a broader sense of connected community that includes not just healthcare organizations, but social service organizations, such as schools and civic organizations and community-based organizations (CBOs) like neighborhood food pantries and temporary housing facilities.
A true CCC links together local healthcare providers along with a wide array of CBOs, faith-based organizations and civic entities to help address those social factors, such as education, income security, food access, and behavioral support networks, which can influence a population’s risk for illness or disease.
Addressing these factors in connection with traditional medical care can reduce disease risk and advance whole person care. Such is the case in Dallas, Texas, where the Dallas CCC information exchange platform has been operating since 2012. Designed to electronically bring together local healthcare systems, clinicians, and ancillary providers with over a hundred CBOs, the Dallas CCC provides a real-time referral and communication platform with a sophisticated care management system designed and built by the Parkland Center for Clinical Innovation (PCCI) and Pieces Technologies, Inc.
Long before this information exchange platform was implemented, the framers of the Dallas CCC came together to consider whether Dallas needed such a network and whether the potential partners in the community were truly ready to make the commitments needed to bring this idea to fruition.
As more and more communities and healthcare provider entities realize the tremendous potential of addressing the social determinants of health by bringing together healthcare entities and CBOs and other social-service organizations, the question of community readiness for a CCC is being asked much more often. But how do you know what the right answer is?
Before looking at the details of how we might answer this, let’s remember that a CCC doesn’t don’t just happen in a vacuum. It requires belief, vision, commitment? and above all? alignment among the key stakeholders. Every CCC that has formed, including the Dallas CCC, begins with a vision for a healthier community and its citizens.
This vision is typically shared by two or more large and influential key community stakeholders, such as a large healthcare system, school district, civic entity, or social- service organization like the United Way or Salvation Army. Leaders from these organizations often initially connect at informal social gatherings and advance the idea of what if?
These informal exchanges soon lead to a more formal meeting where the topic is more fully discussed and each of the participants articulates their vision for a healthier community and what that might look like going forward. This stage in the evolution of a CCC is perhaps the key step in the transformation process, as while all stakeholders will have a vision, achieving alignment among those visions is no small feat.
Many hopeful CCCs never pass this stage, as the stakeholders cannot come to agreement on a common vision that each can support. For the fortunate few, intrinsic organizational differences can be successfully set aside to allow the CCC to move forward.
It is encouraging to see many healthcare systems and payors focusing on the impact of social determinants of health (SDoH) and looking for ways to partner with community-based organizations to address and improve these issues locally. Although this is a necessary step, I believe that providing access or referrals to community organizations is not the full answer.
While healthcare systems can provide referrals and connect patients to resources such as food banks or employment resources, it may not be enough to create individual engagement and empowerment to use those resources. We more fully need to appreciate the role played by the environment in which we grow up and the choices available to us in shaping how we respond toSDoH factors as individuals.
As part of an innovation center where we align data science withSDoH to help systematically disadvantaged individuals, I’ve been witness to projects and research that point to the theory of individual resiliency as part of the equation. The American Psychological Association defines individual-level resilience as the process of adapting well in the face of adversity, trauma, tragedy or threats.[1]
A review of the research on resilience by the WHO found that an individual’s ability to successfully cope in the face of significant adversity develops and changes over time, and that interventions to strengthen resilience are more effective when supported by environments that promote and protect population health and well-being. Further, supportive environments are essential for people to increase control over the determinants of their health.[2]
Also, in addition to traditional resilience methods, the emergence of methods to assess an individual’s capacity for self-care are adding significant insights into personal determinants of health. In particular, the needs of the growing population of complex patients with multiple chronic conditions calls for a different approach to care.
Clinical teams need to acknowledge, respect and support the work that patients do and the capacity they mobilize to enact this work, and to adapt and self-manage. Further, clinical teams need to ensure that social and community workers and public health policy advocates are part of the proposed solution. Researchers at the Mayo Knowledge and Evaluation Research (KER) Unit and the Minimally Disruptive Medicine (MDM) program led by Dr. Kasey Boehmer are developing qualitative methods and measures of capacity and individual’s ability for self-care.
Take post-traumatic stress disorder (PTSD), as an example. It has been estimated that around 50-60 percent of people in the US will experience severe trauma at some time in their lives. Around one in 10 goes on to develop PTSD, which is permanent in a third of cases.
But some people who have lived through major traumatic events display an astonishing capacity to recover.[3] A complex set of factors can be attributed increasing an individual’s resiliency to trauma including their personality, their individual biology, childhood experiences and parental responses, their economic and social environment as shaped by public policy, and support from family and friends.
Addressing the social determinants of health (SDoH) in communities is a hot topic of conversation in healthcare. The industry has bought into the theory that 20 percent of an individual’s health is determined by clinical care and the rest by social, economic, genetic and behavioral factors. But perhaps more importantly health systems need to recognize that they can’t solve this issue on their own.
From my perspective at PCCI, I’ve seen an increase in value-based contracting models in recent years, and health systems and physicians are looking beyond the four walls of their institutions to build relationships with outpatient, behavioral health, post-acute care, and now non-medical providers. The number and types of collaboratives between health systems and non-traditional providers has been growing over the past several years with a recent report gathering information on more than 200 different partnerships between hospital and community-based organizations across the country.
But while health systems may be embracing community provider relationships, I believe that sustainable success in addressing social determinants of health requires a fundamental shift in the way health systems view their role in improving the health of their communities.
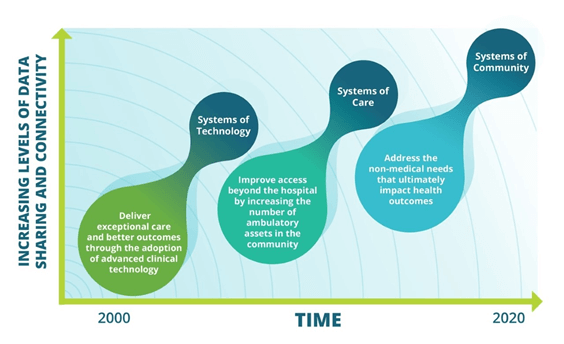
Over the past ten to fifteen years there has been an evolution in how health systems have approached improving health outcomes. Initially health systems focused on providing high-tech solutions for care delivery such as robotic surgery, and advanced imaging techniques. Then to meet the need for increased access and demand for outpatient services, health systems seeded service areas with ambulatory surgery centers, urgent care, retail clinics, and physician offices.
In each of these evolutions the strategies centered on a solution created by the health system alone. And one could argue that the main beneficiaries of these investments were often the health systems themselves – increased market share, improved reimbursements. But such a self-centered approach will not work when addressing social determinants where the root causes lie outside the four walls of the health system.
Effectively creating a system of community will require a collaborative mentality from health systems. While they may have power and influence to gather partners to the table, execution of successful interventions lies with social services and community-based organizations that are the experts in understanding and helping individuals address social needs. Even if not leading, health systems should still be active participants in this work. Indeed, there are areas where their contributions to the organization of partners is critical:
The term “social determinants of health” is far more than a trendy new buzzword in health care. Serving the physical, mental and social needs of the community is not just the right thing to do but can mean substantial improvement in care and reduction in unnecessary healthcare costs.
Several studies have shown that addressing social needs, such as food or housing insecurity, can have a significant impact on a person’s healthcare outcomes and costs. Individuals experiencing housing insecurity or homelessness have higher rates of chronic diseases such as high blood pressure, heart disease, diabetes, asthma, chronic bronchitis, and HIV. This in turn leads to higher utilization of healthcare services such as emergency room visits, inpatient hospitalization and longer lengths of stay compared to those individuals with secure housing. Similar results are seen in those experiencing food insecurity.
Hospitals often state that part of their mission is to provide high quality care and improve the community’s health, or community benefit. A recent study of hospital mission statements in three states (Ohio, Florida and Texas) found that while quality was cited most often (65%), the second most frequently used term was community benefit (24%).[1] If community benefit or community health is part of your health system’s mission statement, how much are you really doing to address the whole health of a community vs. just addressing their “sickness” needs?
At PCCI, our combination of data scientists and expert clinicians believe that health systems have an obligation to address social determinants of health to ultimately remove the disparities and inequality that we see in our community’s health. Yet this is tricky because success requires outreach skills, community relationships and data insights that extend beyond the traditional promise of health-related services. That said, there are three key elements that can assist health systems in making an investment in social determinants of health a reality. To move from theory to action, my suggestion is that health systems do the following:
Leverage the board’s community presence to align on areas of greatest need
As part of health system leadership, board members ensure alignment between mission and a defined SDoH strategy at all levels of the organization. As community representatives themselves, board members can also create the momentum and connections that health systems need to bring community and business partners together to create a governance structure for launching a connected community of care. Such governance structure will guide the strategy, legal and policy needs, and the investment and execution of a connected and aligned SDoH strategy.
Invest in long-term partnerships to ensure sustainability
Recognize that as health systems, you alone cannot solve for social determinants. To truly meet the social, behavioral and emotional needs of some of the most vulnerable individuals in your community, you need to identify community partners with expertise in these areas. With the assistance of board members, assemble a partnership collaborative, with a formal governance structure, to build community-based strategies around SDoH needs. Support the sustainability of this collaborative with technology and data science techniques to identify specific root causes of social need in target populations, share data, and measure impact of interventions. Identify an independent partner to evaluate the effectively of the SDoH initiatives and measure the cost, savings and impact across the community and for the health system.
Parkland Center for Clinical Innovation (PCCI), which improves healthcare for vulnerable populations with advanced data science and clinical expertise, has developed a predictive model that in two years has helped prevent more than 2,000 adverse drug events (ADEs) for hospitalized patients, delivering a potential savings of more than $17 million by reducing re-admissions and eliminating ADEs.
The program, Patients at Risk for Adverse Drug Events (PARADE), is a partnership between PCCI and Parkland Health & Hospital System. During the two years of implementation, PARADE has demonstrated positive results combating ADEs, a problem that impacts more than 450,000 patients nationwide and increases the risk for re-admissions, lengthens the stay of patients by two to three days and adds almost $4 billion in extra hospital costs annually. The most common drug classes associated with ADEs include anticoagulants, diabetes medications, and opioids.
PARADE screens all adult patients at the point of hospitalization and flags high risk individuals who can benefit from pharmacist intervention. To score a patient’s level of risk, PARADE captures a patient’s medical history, including medications and disease complexity, prior healthcare utilization, demographics and social determinants of health. It then provides results in real-time, with seamless integration into a patient’s electronic health record.
During its two years of implementation at Parkland, the PARADE program has screened more than 87,000 patients, with 8,731 high-risk patients identified. Of the high-risk patients, 16 percent received timely pharmacy intervention and more than 2,000 ADEs were prevented. For high-risk patients receiving a consult, the 30-day re-admission rate was cut by 23.5 percent.
“Close collaboration with Parkland’s front-line pharmacy team from idea to implementation has been critical for the success of PARADE,” said Manjula Julka, MD, PCCI’s vice president, clinical innovation. “PARADE has proven to improve quality of care by helping the pharmacy team to identify and intervene with high risk patients within 24 to 48 hours of admission. Upwards of 50 percent of ADEs are detectable and preventable and PARADE gives us a potent tool to help hospitals stay ahead of a difficult problem that causes longer stays and drives significant costs for hospitals.”
Kristin Alvarez, PharmD, BCPS, Associate Director Clinical Advancement/Best Practices for Parkland and Brett Moran, MD, Chief Medical Informatics Officer for Parkland, led implementation of PARADE at Parkland. Due to the model’s high accuracy and real-time user-friendly information, Parkland has adopted PARADE as a primary tool for pharmacist daily workflow for consult identification with demonstrated impact on preventing potential ADEs.
PCCI’s strategic partner Pieces Technology, Inc. is supporting the commercial deployment of PARADE and other similar models.