What is that one factor that separates one patient from another? Can one identify why two patients with the same illness but from different regions respond differently to a particular treatment? Do we need to cater to the needs of patients even after they leave the clinic?
These questions have always intrigued not only the physicians but every member who is involved in the care journey— care teams, communities, social workers, even patients themselves. And the answer lies in just one fact— even if these two patients appeared similar on paper, their lifestyles are very likely to differ: socioeconomic status, gender, race, ethnicity, family structure, and education.
All of this comes down to just one term: Social Determinants of Health.
This is one of the prime problems that has kept healthcare organizations in a situation of dilemma.
We are way past the statement that SDoH is just another hype
Have you ever tried to score a home run with one hand tied behind your back? This situation is similar to the condition of healthcare organizations in the value-based ecosystem. They are trying to get 100% of the task of healing a patient done with just 50% of the insights.
Social determinants matter because they can affect the health of the population residing in a particular region, for better or for worse. We have countless studies that show the importance of social determinants, yet we are not able to properly address them because we are not able to answer these questions:
How do we address the challenges that we don’t even know exist?
Who is responsible for addressing these challenges?
Is there any ideal strategy to address SDoH?
No matter how famous they are in healthcare, working with SDoH requires a drilled-down approach and something that we have in abundance- healthcare data. This data can be leveraged, and with the use of predictive analytics, organizations can accurately measure the at-risk population and advance preventive care methods in the ecosystem.
The best way, I think, is to look at this picture with a magnifying glass. Traditionally, the endpoint is the state-level analysis of SDoH. However, it is not the end but the beginning of the study that should go to the zip code level.
Here are some of the most interesting stories of how the leaders in the field of addressing the Social Determinants of Health addressed the populations’ needs and did the undoable.
What was the Humana way to deal with the non-clinical factors?
Humana has the Bold Goal Initiative, which is a population health strategy that is aimed at improving the health of the communities and making them 20% healthier by the year 2020. Their Healthy Days surveillance process is a robust and scalable metric. Based on this, they found that food insecurity and loneliness were among the top contributors to the total unhealthy days among the population they serve.
With their holistic and comprehensive approach, they built an analytic intervention pipeline to address these issues. One instance is their intervention with Papa Inc., where they connected college kids to seniors who needed companionship. As a result, 94% of members stated that the Papa Program helped them to feel more socially connected.
Humana was able to reduce the number of unhealthy days from 2015 to 2018 by simply addressing the non-clinical aspects of care delivery for their population.
Performance of Humana’s seven original Bold Goal communities (2015-2018) – Humana Medicare Advantage members
How MercyOne PHSO took the understanding of non-clinical factors from the zip code level to an individual patient level?
MercyOne PHSO, one of the largest ACOs in the Midwest, wanted to know the factors affecting their patients. They took the simple concept of asking the right questions and leveraged it to understand their patients.
While their patients entered the hospital or examination room, they asked them to complete a survey consisting of questions that depict the factors that affect their patients’ health, such as:
In the last 12 months, were you worried that your food would run out before you got money to buy more?
What is your living conditions today?
Do you face any difficulty in reaching out to your doctor?
Imagine your favorite football team is in a real neck-to-neck with another team, and the game could tip in anyone’s favor. It is the last minute, and in an insane turn of events, the quarterback throws the ball in the air, hoping the player in the end zone could make a touchdown. Instead, the reckless throw results in confusion, the guy in the end zone gets tackled, and the game ends in disappointment.
Now, let’s step out of football and look at these statistics that show a little picture of referrals in healthcare:
Only about 50% of referrals result in a completed appointment
Less than 25% of referrals are completed as intended by the referring provider
In case one, the player didn’t score a touchdown, and in the second case, the patient didn’t end up with the right provider and the treatment. The reason being the process— a reckless throw and an inefficient referral procedure.
Most healthcare organizations lose about 30% to 60% of patients on account of inefficient referrals. Value-based care is expected to become the leading payment model by the year 2020, and healthcare organizations cannot afford losing more than half of their revenues due to reduced referral leakages.
How do you know that your referral management needs healing?
Imagine a situation where a patient, in his early 60s, suddenly suffers from severe abdominal pain. He goes to his doctor, and the doctor directs him to a specialist she knew out of her professional knowledge.
Now the situation can unfold in many ways, where the patient might end up getting treated or the exact opposite of it. In all the scenarios, the part where things might go wrong is the process of referring the patient. The problems that these stakeholders might face include:
The inability to identify in-network providers
Lack of proper patient information
Limited access to information flow among providers
Reliance on age-old techniques of fax-based referrals
… and many more.
Now the question is: ‘What is the solution?’
It all boils down to just one thing— having the right data. Imagine you visit your doctor. The moment you tell him your problem, he looks into his screen to look for the right specialist. In just one click, he gets all the correct specialists in a listicle format. And all he has to do for the rest of the story is just click on the ‘Refer’ button.
Seems undoable? Actually, all we need is a data-driven strategy.
Don’t just plan your data but also your approach
It is never about just knowing the patients but understanding them, their health, their socio-economic condition, and their care journeys. All of this is not possible if we do not have access to the right data. Whether it be a lab test or spiking blood pressure— nothing should be left undetected.
Easier it is for providers to understand, efficient will be the referral
You cannot expect the rest of the process to be perfect if the beginning is imperfect. If the provider is stuck finding the information, not only will this delay the referral but also increase the chances of errors. What they need is a single screen view of specialists in a list that includes every detail such as geography, specialist ranking, availability, and fees, among others.
Connecting communities and care teams to deliver the best care
It is crucial that care teams and communities remain aware of the events happening in the patients’ care journeys. They need a streamlined tracking of patient referrals at the clinical or patient level. It will reduce the turnaround time for escalations.
The patient lost in the process is the revenue lost
The right referral strategy includes two significant aspects:
Increasing the visibility into the process to the patient
Using advanced analytics tools to develop a lens into the referral process
What they need is a simple reminder that enlists all the details regarding the visit and gives timely updates to them regarding the specialist and the appointment date. Organizations can increase patients’ access to telehealth services by allowing plans to propose the use of telehealth services instead of promoting in-person visits.
The healthcare circles in the United States are reeled up by debates around the need for price transparency.
The federal agencies are coming up with regulations.
Healthcare associations are weighing in their concerns.
Physicians, patients, and economists – everyone is articulating the pros and cons in a rather plausible manner.
Wait. What has triggered this rush towards transparency?
To begin with, the healthcare costs across the country have gone from “extreme” to “unreal” in the last two to three decades. A regular MRI scan, for instance, costs twice as much as it does in Switzerland, another country where healthcare is considered “notably expensive.”
Worse still, one simply cannot tell how much money they might end up paying at a healthcare facility at any given point. A broken bone can take thousands of dollars to get fixed or at no cost at all – depending on a dozen factors that can vary drastically with each patient.
Frankly, there is no single moment that burst the bubble around the soaring healthcare costs. In many cases, what hurt patients more than the total cost of a procedure is the out-of-pocket expense that they are made to pay. The focus today has shifted to one fundamental question – how much money is justified for a given care procedure; and are we entitled to know it or not?
Cut to 2019, a movement to make care prices transparent is shaking the establishments across the US.
What is the government saying?
The government has taken the onus of ensuring transparency in healthcare prices. Last month, the White House issued an executive order aimed at making payers and providers publish the cost of each procedure available at their facility. The government believes that this step can get a long way in making patients take more informed decisions regarding their health and eliminate the opacity regarding the cost associated with such processes beforehand.
The intent here is to provide patients “access to useful price and quality information and the incentives to find low-cost, high-quality care,” something that can be a giant leap forward in the direction of enabling cost-effective care.
One of the greatest challenges in healthcare is keeping up with the changing landscape. Considering only since the beginning of 2019, the Centers for Medicare and Medicaid Services (CMS) and other federal agencies, such as the Office of National Coordinator of Health IT (ONC) and the Department of Health and Human Services (HHS), have introduced a number of rules as a measure of upholding their goal of empowering patients and enhancing healthcare efficiency. We’re at a very critical juncture in healthcare and from a regulatory perspective, there are a few key rules that merit a special focus which will have a great impact from both a clinical and financial standpoint.
The MyHealthEData Initiative in 2019
The MyHealthEData initiative, launched in March 2018, aims to “empower patients by ensuring that they control their healthcare data and can decide how their data is going to be used, all while keeping that information safe and secure.” Only a few days back, CMS upped the ante for better data access by expanding this initiative and announcing the pilot of “Data at the Point of Care.”
The Data at the Point of Care (DPC) pilot will be connecting providers with Blue Button data, where providers can access claims data to learn more about their patients and their previous diagnoses, procedures, and prescriptions. While providers had to comb through several hundred data sets previously, the DPC program would aim to make access to data easier and right within their workflows.
This announcement follows the relaunch of the Blue Button initiative, or Blue Button 2.0, that grants access to health data and enables patients to send that information using FHIR-based healthcare apps.
In a nutshell, these moves come as an overall push from CMS to promote better access to data and 100% healthcare interoperability. In addition to enabling data access, CMS has also been targeting information blocking, as reflected by 2019 MyHealthEData updates. With these measures, both patients and providers will have the required insights to make more informed healthcare decisions.
The Trusted Exchange Framework and Common Agreement
In April 2019, ONC published its second draft of the Trusted Exchange Framework and Common Agreement (TEFCA), focusing on three high-level goals:
Providing a single ‘on-ramp’ to nationwide connectivity
Enabling Electronic Health Information (EHI) to securely follow the patient wherever needed
Supporting nationwide scalability
TEFCA is basically a common set of principles which serve as “rules of the road” for nationwide electronic health information exchange across disparate health information networks (HINs). The framework, which was mandated by the 21st Century Cures Act, provides a set of policies and procedures along with technical standards required to enable healthcare data exchange among providers, state and regional HINs, and federal agencies.
By Abhinav Shashank, CEO and co-founder, Innovaccer.
Fact 1: As per the latest data made available by the Office for Civil Rights for HHS, more than 208,000 privacy-related complaints have been made in the last 16 years.
Fact 2: If a hospital makes a call to a patient
to remind them of their upcoming appointment, they might receive a class action
complaint about violating the Telephone Consumer Protection Act.
While
these two facts may not necessarily be related to one another, we clearly need
to take a hard look at the increasing calls to protect patient privacy. But
does that mean providers cannot send a text message to their patients?
Certainly not!
California’s latest policy for text
message technology for Medicaid plans: A case study
The
1991 Telephone Consumer Protection Act (TCPA), which was put in place to
safeguard people from automated text or other telephonic messages, limits
organizations from reaching out to their patients through text messages. TCPA
can also levy financial penalties on organizations if they are found guilty of
violating their policies. On the other hand, the Health Insurance Portability
and Accountability Act of 1996, or HIPAA, require every “Covered Entity or
Business Associate that comes into contact with Protected Health Information
(PHI)” to follow the compliance policies, something that is accepted as a rule
of thumb in the healthcare world. For any organization looking to reach out to
patients remotely, both HIPAA and TCPA policies are extremely important to
comprehend and follow.
In
today’s context where patient engagement through text messages has emerged as
one of the biggest avenues for optimizing care quality, the TCPA is losing its
sheen to some extent in the healthcare domain. While no one denies the
importance of TCPA, it does cause some roadblocks for organizations looking to
enhance patient engagement in remote areas and population segments.
The
California Department of Health Care Services (DHCS) recently issued a policy
to set guidelines regarding how Medicaid plans can safely use the text
messaging technology to connect with beneficiaries. This is critical since one
out of three people in California are Medicaid beneficiaries.
The
latest ruling allows organizations to reach out to their patients through text
messaging after submitting an approval form to the concerned regulators clearly
mentioning the structure as well as the intent of such reach out campaigns.
They also need to create proper avenues for privacy protection and give users a
clear opt-out option. However, once such campaigns are approved, the payer can
then run such programs without any additional regulatory clearances. Further,
such outreach messages must be made available at no cost to Medicaid members.
What can we learn from the example of
DHCS?
According to a study, hospitals could reduce their discharge time by 50 percent if conducted by secure text messaging, saving healthcare facilities an average of $557,253 per year.
Secure
text messaging is indeed a big deal. Make no mistakes, privacy and security
should still remain the top-most priority while enabling such mechanisms, and
password protection is something that we should all consider. However, in an
age when we are shifting our focus on precision medicine and advanced robotic
surgeries, the ability to create a secure system for text reminders should not
be a big deal.
The
text message service is indeed the most prevalent form of communication for Americans
younger than 50, and about 80% of people state it as the preferred way of receiving
notifications. The latest DHCS policy will empower payers to connect with their
populations like never before, an ability that would allow them to initiative
preventive care and scheduling, while ultimately reducing care and cost and
improving outcomes. It can be safely assumed that the latest initiative by DHCS
is a breakthrough step in this direction.
Organizations need the ability to meet
their patients where they want
I
remember one of my friends asking me a very simple yet important question, “If
I can connect with my colleague based out of London in literally 10 seconds,
why does it take my provider so long to tell me that my appointment has been
canceled?” I had no answer.
We
cannot expect a person whose calendar is booked for the next 10 days to walk
into a clinic for a regular check-up and wait idly for a couple of hours due to
inefficient scheduling practices. Worse still, imagine a situation where a
person takes time out to visit a facility for their Annual Wellness Visit (AWV)
only to find out that their appointment has been rescheduled for the next week.
A simple suggestion of taking aspirin as a first-aid measure in a potential case of a heart attack sent through an SMS on your way to the hospital can help a patient significantly reduce the damage. Remote patient outreach is an important prospect for today’s practices, if not a necessity. It’s really that simple — connect with your patients to know them better, to treat them better, and to make them feel better with minimum interventions. While organizations can still sustain under value-driven contracts without such streamlined patient communication mediums, we cannot keep believing that we would cross that bridge when we come to it.
The road ahead
Consumerism
in healthcare was never a widely-discussed topic until very recently, however,
things are changing and how! Innovating while respecting the mandates in place
should be the road ahead, definitely. The government is supporting new-age
initiatives, federal healthcare agencies are bringing in new policies, and
large payer and provider organizations are exploring ways to maximize patient
satisfaction. Examples set by organizations such as DHCS will act as an ice
breaker for other agencies and organizations wanting to break free to cater to
the unique needs of the 2020s.
By Abhinav Shashank, CEO and co-founder, Innovaccer.
Abhinav Shashank
The Johnsons were blessed with twins the day before; two healthy baby boys, haphazardly named Jill and John in the health records. Definitely, this marks the start of pediatric services in the family. Hospital records set for the twins hardly mark any difference, gender, weight, parents, address; all records read the same. The only visible difference is a skin allergy with the second baby.
Their names were changed to Jack and Ross in a
month, and records got multiplied by two. Vaccinations done within the first
month were registered in the records of Jill and John, while Jack and Daniel
got registered under fresh EHRs.
Is the
pediatric space ripe enough for Machine Learning?
How should the healthcare industry deal with
data redundancy or data hop, and maintain data integrity to ensure reliable
records? This is a real serious concern for pediatric organizations.
However, to our rescue is machine learning technology aiding the critical issue of record matching and streamlining medical procedures in child healthcare. ML has the potential to revolutionize the pediatric care ecosystem and assist the major challenges in healthcare operations of the young population.
With the global healthcare market estimated to reach a sweeping $11,908 billion by 2022 and fast-growing problems in the younger population, there is certainly a vast frame of exploration for pediatric focus and care delivery for the young. Being a continuously evolving age group with tailored and sensitive healthcare needs at different stages of growth, the pediatric population is most challenged when it comes to successful reforms and insights.
How are
EHRs doing injustice to the future of healthcare?
Kids from their birthdate are expected to face the EHR duplicity that scatters their record and essential medical data. The key facts of a newborn like weight, height, allergies, among others, are stored in an EHR that is occasionally hopped a month later, with a permanent name signing in.
Once a new EHR is registered with the new name, all medical information of the previous few months gets disconnected. This has a challenging impact on the entire care protocol. The critical notch here is incoherent vaccination and immunization information of the growing baby. Not only does it lead to seemingly real care gaps, but also ripples out to erroneous procedures and increased health costs.
Machine Learning is transforming the way
services are delivered globally. Detecting the minutest of factors in an
outcome, and cascading the learning over huge data, it can provide us with
crucial considerations which are evidently present but still go unnoticed by
us. ML is helping to deliver accurate algorithms for all domains. Applying ML
to pediatric care is sure to transform the current scenario of care delivery
for the younger population.
What
are the major challenges pediatric organizations are facing?
We need strict adherence and care, not only to
ensure healthy children but also to ensure optimized care procedures for them
in the future. However, there are a lot of shortcomings in understanding and
implementation of the medical requirements of the population aged 0 to 18.
The major challenges in this regard are:
Most pediatric organizations today do not have precise and distinct health measures to evaluate the younger population. We need measures that can efficiently assess the patients on their growth-specific checkers, respectively.
Patient records at different stages are difficult to merge, with inadequate data-merging proficiency.
Data hop in EHRs during record matching or establishment. This is of critical concern for babies and toddlers who need consistent care episodes.
Lack of customized reach to parents for time-sensitive immunization and vaccinations. This leads to missed appointments, which leads to complications and increased costs over time.
Care plans including uncertainties to manage intelligent adherence. This will enable strong network functionality and improved care.
Flexible and optimized timeline for care delivery.
Currently, about 50 percent of children under five years of age attend out of home care. Throughout childhood, children receive care at daycares, check-ups at community places, have physician visits at different pediatric facilities, among others.
It becomes essential to compile entire patient data at a single place to avoid redundant and erroneous procedures. According to the American Health Information Management Association, an average hospital has about a 10 percent duplication rate of patient records. A study by Smart Card Alliance in 2014 projected that about 195,000 deaths occur yearly in the US because of medical error, with 58 percent of them being associated with “incorrect patient” errors.
Does
Machine Learning truly have the answer?
An article in the AAP News and Journals Gateway mentions that only 71.6 percent of young children in the United States have completed their primary immunization series. Moreover, evidence suggests that 10 percent to 20 percent of young children receive more than one unnecessary and extra immunization. Evidently, scattered records lead to a lack of timely, accurate and complete immunization. This can have serious repercussions on the health and care protocol of the patient, in addition to increased medical costs.
Machine Learning can nourish the split needs
and resolve the errors of pediatric healthcare in different domains:
Automatic Triggering for Episodes and Immunization: ML algorithms can be developed to track and prompt parents for necessary episodes and immunization. This will ensure timely care episodes.
EMPI Matching: Enterprise Master Patient Index is a database of medical data across departments and healthcare organizations. Machines trained in pediatric EHRs can develop a robust algorithm to match patient records across hospitals and unify them.
Streamlining Vaccinations: ML algorithms can regularize time-sensitive vaccination arrays for different pediatric categories as decided by the World Health Organization.
Scanning Data Hops: ML algorithms can detect data gaps in procedures, and point out critical consequences enforcing timely merging of EHRs.
Predicting Episodes and Costs: ML algorithms trained with localized pediatric data can detect underlying factors for an episode and predict the average costs for unforeseen episodes.
The
road ahead
The pediatric population is foundational to a
healthy nation and demands our attention to reform its split functionalities.
Machine Learning can bring about unimaginable amendments in our current
pediatric care management and delivery. Data, which is foundational to all
ventures in the healthcare industry, can be merged with ML to close all care
gaps and invest in a healthy tomorrow.
The world of healthcare is changing and those changes impact how we deliver care, our approach to engaging patients and the relationships between stakeholders across the healthcare value chain. Each day, we witness advances in genomics, imaging and pharmacology, and learn about the use of artificial intelligence (AI) to drive these advances. Indeed, healthcare is in the midst of a major revolution and AI seems to be at the very core of this transformation. How much of the AI story is hype and how much is real?
Innovaccer Inc., a San Francisco-based healthcare data activation company, is hosting a breakthrough AI webinar on June 20 with guest speakers Dr. Peter Lee, corporate vice president, Microsoft Healthcare, and Stephen K. Klasko MD, MBA, president and CEO, Thomas Jefferson University and Jefferson Health, who will be discussing the new healthcare domains of AI, and it’s “never imagined” impact. They will be joined by webinar moderator, David Nace MD, chief medical officer at Innovaccer.
The use of AI in healthcare has lagged behind other industries, in large part because of the lack of comprehensive, pristine data. The webinar, titled “Beyond Interoperability: Data Activation and Artificial Intelligence for Healthcare,” will focus on the recent AI hype, tease fact from fiction, and explain how advances in data activation can solve the accuracy and interoperability problems in the space.
Dr. Lee has extensive experience in managing the process of going from basic research to commercial impact. Past illustrative examples include the deep neural networks for simultaneous language translation in Skype, next-generation IoT technologies, and innovative silicon and post-silicon computer architectures for Microsoft’s cloud. He also has a history of advancing more “out of the box” technical efforts, such as experimental under-sea data centers, augmented-reality experiences for HoloLens and VR devices, digital storage in DNA, and social chatbots such as XiaoIce and Tay.
Lee is a member of the board of directors for the Allen Institute for Artificial Intelligence and the Kaiser Permanente School of Medicine. He served on President’s Commission on Enhancing National Cybersecurity. And, previously, as an office director at DARPA, he led efforts that created operational capabilities in advanced machine learning, crowdsourcing, and big-data analytics, such as the DARPA Network Challenge and Nexus 7.
Under Dr. Klasko’s leadership, Jefferson Health has grown from three hospitals in 2015 to 14 hospitals today. His 2017 merger of Thomas Jefferson University with Philadelphia University created a pre-eminent professional university that includes top-20 programs in fashion, design and health professions, coupled with the first design-thinking curriculum in a medical school, conducting the nation’s leading research on empathy, an essential component of medicinal practice that is often overlooked in the academic setting. As a disruptive leader in the academic ecosystem, Dr. Klasko brings a valuable point of view to the Innovaccer Strategic Advisory Council.
By Abhinav Shashank, co-founder and CEO, Innovaccer.
Abhinav Shashank
While healthcare leaders uniformly agree that transitioning to value is the way healthcare is going to be in the coming days, it is unclear to most how they can make the transition without negatively impacting their cost outcomes. In an industry which had primarily been fee-for-service based, healthcare organizations are facing immense pressure to innovate and adapt or risk their long-term viability.
In developing strategies to succeed with these trends, many healthcare leaders are realizing that Medicare Advantage (MA) is a key component to their long-term success. The Centers for Medicare and Medicaid Services (CMS) has projected that Medicare Advantage enrollment will reach an “all-time high” in 2019 with 22.6 million Medicare beneficiaries, given the unprecedented growth. And industry analysts like L.E.K. Consulting say that Medicare Advantage enrollment will rise to 38 million, or 50 percent market penetration by the end of 2025.
Going along the same lines of ensuring long-term success and enhanced patient satisfaction, CMS rates Medicare Advantage plans by giving them Star Ratings which help beneficiaries and their family members make informed decisions. As MA Star Ratings become the most visible mark of success, the only trail of thoughts would be: How to improve these Star Ratings?
How do Star Ratings work?
The Medicare Star Ratings are key measures of the quality of care a health plan provides. The health plans are rated on 45 measures categorized under five categories which portray how a health plan takes care of its beneficiaries.
Needless to say, there’s a lot at stake here. The more Stars a health plan has, the more likely they are to attract beneficiaries. But earning top ratings is a difficult task. Payers that wish to reap the benefits of high Star Ratings also need to deliver impeccable care to their members and ensure a satisfactory experience of care.
What holds MA Plans back from achieving better Star Ratings?
A majority of these measures are defined on the basis of specific service received, claims, or clinical information that verifies access and delivery of care. For example, if there is a large number of members that have a chronic disease, plans can pinpoint them and identify the specific care they have received during the year. After that, they can plan targeted interventions to close the gaps and be on the path to deliver positive outcomes.
However, with limited actionable member data available, MA plans just end up focusing on broad, general interventions as compared to undertaking a member-specific, targeted approach. MA plans require timely and detailed information about their members’ health to create interventions that have a lasting impact.
Additionally, it’s important to realize that beneficiaries don’t just have high-quality care, but also have quick access to healthcare service. MA plans need to ensure that the quality of care is always upheld. In most cases, it stems out of efficient collaboration between the clinical staff and healthcare technology.
More importantly, improvements in Star Ratings depend significantly on how engaged a patient is. For example, measures which are related to medication adherence are almost completely hinged on strong patient engagement that makes it easier for patients to get access to their medications and take them on time. In other words, MA Plans need to deploy efforts that are aimed at implementing holistic strategies to address patient needs.
 Is there any ideal strategy to address SDoH?
Is there any ideal strategy to address SDoH? 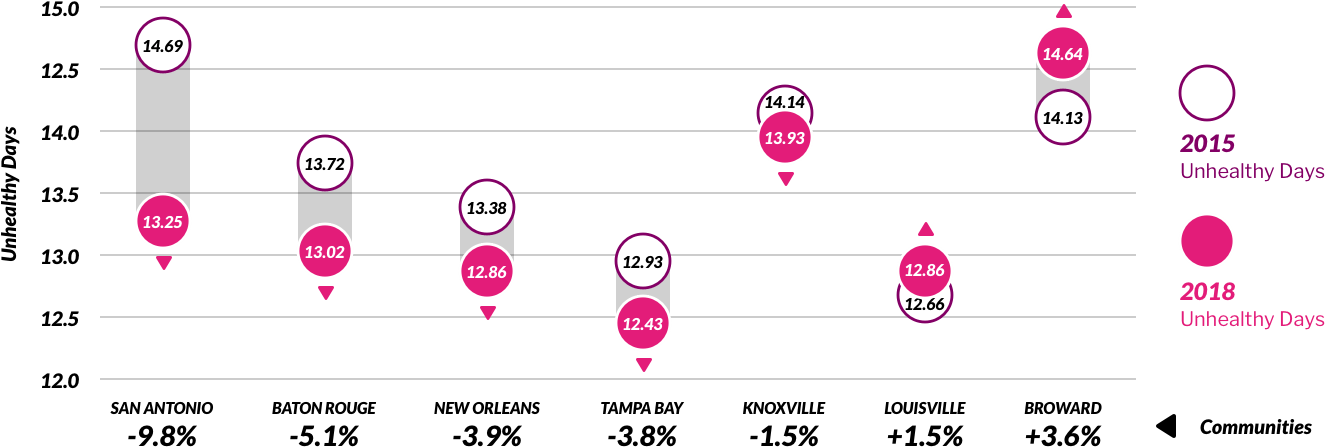
 Imagine your favorite football team is in a real neck-to-neck with another team, and the game could tip in anyone’s favor. It is the last minute, and in an insane turn of events, the quarterback throws the ball in the air, hoping the player in the end zone could make a touchdown. Instead, the reckless throw results in confusion, the guy in the end zone gets tackled, and the game ends in disappointment.
Imagine your favorite football team is in a real neck-to-neck with another team, and the game could tip in anyone’s favor. It is the last minute, and in an insane turn of events, the quarterback throws the ball in the air, hoping the player in the end zone could make a touchdown. Instead, the reckless throw results in confusion, the guy in the end zone gets tackled, and the game ends in disappointment.