The government is determined to see that all healthcare institutions use electronic health records (EHRs) and electronic medical records (EMRs). Their features, after all, streamline the healthcare process. Many physicians and healthcare professionals, however, remain reluctant to implement these records, overwhelmed by the complex system.
Although inefficient systems can make physicians a “slave” to their EMR/EHR, the software increases workflow efficiency and preserves critical medical information when implemented properly.
EHR and EMR implementation is a costly affair. The software, hardware, implementation assistance, support, training, and ongoing fees consume a large chunk of your planned capital investment.
According to government reports, the minimum cost of purchasing and installing an EHR/EMR system is $15,000, while the maximum is $70,000 (depending on the provider). Unplanned expenses may also add to the total cost of implementation. Finding financial resources for EHR and EMR is a major hurdle, especially for smaller practices.
The software cost is one of the reasons that discourage healthcare institutions from investing in EMR and EHR. Still, the benefits significantly outweigh the implementation expense; getting an EHR/EMR system is more cost-effective in the long term.
By Anne Dabrow Woods, DNP, RN, CRNP, ANP-BC, AGACNP-BC, FAAN, chief nurse, Wolters Kluwer, Health Learning, Research and Practice.
Anne Dabrow Woods
These are the days we never thought we’d see – unimagined times, pushing our nurses and healthcare workers to the brink with the demands of COVID-19. They’ve stepped up with unbelievable courage and resiliency. They’ve done so without many of the resources they’ve traditionally had, such as personal protective equipment (PPE) and medical equipment. But one thing that’s undoubtedly made a difference is technology.
Patients have been able to interact with their primary care provider and nurses via telehealth ensuring that patients are able to continue with the medications and treatment plans for chronic conditions and new issues.
In the acute care space, it has enabled patients to visit with their family through digital technology, and providers and nurses have been able to update the families on patients’ progress.
After patients are discharged with COVID-19, the patient is in daily contact with a nurse to make sure their condition isn’t worsening, and they understand how to care for themselves. This works to ensure patients have follow-up care and the family is supported. And those are just a few ways.
While the survey was taken prior to the pandemic, the results give insight into the role of technology as it applies to both next-generation nurses (those with less than 10 years of practice) and more experienced ones. The survey conducted by Wolters Kluwer aimed to explore the mindset of today’s nurses and healthcare workers, so hospitals can respond accordingly.
Digital natives versus techno-phobes
When looking at next-generation nurses, we should keep in mind that many of them grew up in a time with widespread use of the internet, social media, and mobile communication. Many nurses with longer tenure began their careers when the internet was in its infancy and computers weren’t an integral part of a hospital’s operations.
Next-generation nurses are, for the most part, digital natives. That comfort level does tend to influence their opinions: when care is better, next-generation nurses think it’s because of technology. 84% believe clinical-decision support systems at the point of care are making it easier to make the most informed, evidenced-based care decisions.
In addition, 84% feel specialized systems that provide treatment recommendations and integrate with electronic health records (EHRs) have a positive impact on how care is delivered.
Their understanding of technology may be a factor in them spending less time in EHRs than their more seasoned counterparts; 69% report spending too much time in EHRs, compared to 81% of more experienced nurses.
Next-generation nurses are fans of artificial intelligence (AI). 63% say they are optimistic that the use of AI will help providers get the information they need to make better care decisions.
Experienced nurses weren’t as convinced, with only half agreeing that AI will help in making better care decisions. (This insight should alert hospital leaders of the need to educate staff on how AI can improve clinical decision making so that implementation of AI will be viewed as a positive and not as a negative.)
According to a new survey fielded by Definitive Healthcare and sponsored by Dimensional Insight, 90% of hospitals and health systems use the analytics component of their electronic health records (EHRs), with 49% using it exclusively or primarily for analytics. With such widespread use, the technology must be meeting the needs of hospitals and health systems, right?
(Wrong.)
The survey data shows that despite the fact that many hospitals are using EHR analytics, they are also challenged by the technology and give it middling rates when it comes to satisfaction. Let’s look at the survey results in more detail and examine where hospitals and health systems go from here.
Hospitals not highly satisfied with EHR analytics
The survey interviewed 108 healthcare leaders on their experience with EHR analytics. It also asked about their experience with analytics-specific platforms and in-house solutions to serve as a comparison point.
Overall, leaders ranked their satisfaction with EHR analytics as a 5.58 (on a scale of 0-10 with 0 being “extremely dissatisfied” and 10 being “extremely satisfied”). In-house solutions received a satisfaction score of 6.51 (17% higher) and analytics-specific platforms received a score of 6.69 (20% higher).
Leaders feel challenged by technology aspects of EHR analytics. For organizations that are using EHR analytics as their primary analytics tool, they feel challenged by:
The reporting and querying is difficult/slow (43.4%)
The component is not robust or advanced enough (35.8%)
Interoperability (30.2%)
Lack of visualization (28.3%)
User interface is difficult to understand/use (26.4%)
Those that are not using EHR analytics cite similar technology challenges as the reason they are not using the component.
By Abhinav Shashank, CEO and co-founder, Innovaccer.
Children have entirely distinctive needs as compared to adults. Care is delivered to them in a manner entirely different than adults by care teams that hardly ever double-up as providers for the elderly.
Abhinav Shashank
In
fact, we hear numerous stories of organizations that transformed their care
delivery by fabricating children-specific strategies and have been really
successful in doing so. However, very few experts ever discuss how little
thought we put when it comes to developing healthcare technologies tailored to the
specific needs of pediatric organizations.
Do pediatric organizations have the
technology to succeed?
By
2017, more than 95 percent of hospitals had certified EHR technology. However,
these EHRs are heavily adult care centric and may not include measures that are
specific to pediatric populations. In fact, in a recent research piece
conducted on 9,000 pediatric patient safety reports, it was found that about 36 percent of reports were related to EHR
usability issues.
EHR
usability has been one of the underrated issues that we need to address if we
are to build an efficient pediatric landscape. This can be attributed to the
fact that even a slight misjudgment in comprehending the information stored in
EHRs can substantially increase the chances of errors and adverse events. The
issue is all lot serious for pediatric organizations where patients are
extremely sensitive to the care provided to them at any given point of time.
Complicated EHRs can do no good to neither children nor pediatricians.
Why is the EHR usability valid ask for
pediatricians?
Infants
born prematurely have different needs as compared to completely healthy
infants. A 5-year old kid faces problems that a 13-year old teenager does not.
Vaccination once missed can prove costly in the future. A child with Type 1
diabetes may require care plans entirely dissimilar to other children.
Theoretically and practically, each child is unique: from a prematurely-born
child weighing less than a kilogram to an obese 105 kg 14-year-old. The EHR
should be able to ingest all such details with perfection and should provide as
many measures that pediatricians may require.
Consider
twin siblings born on the same day, having an identical vaccination cycle, and
same last name. However, they may react differently to various treatments and
have different weight or gender. If they need some medication, they might be
given different mg/dose prescription. Amidst all this, the care teams have the
onus of ensuring that each exercise is taken care of with utmost precision. For
that, they need powerful EHR systems and alert systems, among other things. In
other words, organizations need advanced decision support systems, an ask that
is only valid to deliver value-focused care.
Doctors need reliable EHRs to understand
the complete picture
More
often than not, there are only two sources of information during any given care
episode — data stored in the EHR and patient’s own words. However,
pediatricians cannot expect much support from their young and very young
patients. For infants, it gets all lot difficult since it gets even harder to
comprehend their symptoms.
For
such patients, EHRs need to tell the complete picture each time lest errors are
bound to happen. Goes without saying, children are more vulnerable to such
errors as compared to any other patient population. Ideally, pediatric
organizations need to have extremely robust, agile, and accurate EHR systems.
However, the situation is far from ideal even at this age and time.
Pediatric organizations need custom-made
EHRs and IT infrastructure
To
begin with, EHRs should have an extremely user-friendly interface, support for
adding or converting charts locally for specific syndromes, extremely precise
dosage range, and capabilities to identify missed or pending vaccination. They
should strictly have a pediatric-specific threshold for each symptom,
treatment, or trait, while also having a feature for identifying copied and
newly-added records. Alerts, as discussed earlier, for potentially wrong data
entry should also be a default feature.
Coupled
with a layer of advanced analytics system on top of their EHRs, pediatricians
can successfully navigate the challenges as they come their way. If pediatric
organizations have a system in place to send regular immunization and wellness
visit reminders, they can both increase adherence rates and reduce potential
risks.
Role-based
access to sensitive patient information and automatic triggers for varying
health trends can further play a substantial role in making care more efficient
for the young. All such steps combined can help us in realizing the dream of
creating the “Internet of Healthcare,” where every stakeholder is connected
with each other and there is a seamless exchange of information at all places
in real-time.
The road ahead
As
we embark upon the journey of creating an “Internet of Healthcare” where
everyone would be connected with everyone, we first need to have quality IT
infrastructure that can make this possible. EHRs are the building block for
such a system. It’s time we add the human touch to such technological
solutions, and take the first step in the direction of reinventing EHRS.
By Susan DeCathelineau, vice president of global healthcare sales and services, Hyland Healthcare.
Susan DeCathelineau
Healthcare interoperability continues to be a critical topic facing healthcare technology leaders. There’s no question that achieving true healthcare interoperability is key to moving the industry forward by enabling the type of information exchange that can streamline workflows, inform clinical decision making and enable precision medicine.
However, much of the current interoperability discussion is focused on ensuring core systems, i.e. Electronic Medical Records (EMRs) are compatible with one another. Yet there is one issue that is largely overlooked: the crucial role of integrating structured data with unstructured patient information.
For example, EMRs are designed to capture and manage structured patient data, and they do that job well. That is to say, they capture content using controlled vocabulary rather than narrative text. But the lack of structured data and standardization in the healthcare industry today creates major issues when sharing EMR content within and across healthcare organizations.
EMRs are not built to natively ingest the plethora of unstructured information that exists on a patient. This unstructured content includes things like diagnostic medical images, clinical documents and notes, visible light images and more. According to many industry estimates, as much as 75 percent of the information that exists on a patient lives outside of core applications like EHRs. Instead, this unstructured content is scattered in a multitude of legacy data silos.
Manage your unstructured clinical content
A recent whitepaper by Signify Research illustrates just how pervasive ineffective management of unstructured content is in today’s health systems, and just how vital this effort is to interoperability initiatives. In the paper, author Steve Holloway explains how the growth of healthcare networks resulting from merger and consolidation activity is driving the need for true interoperability. These ever-larger healthcare enterprises are increasing demand for incoming and outgoing information exchange between a diverse ecosystem of providers, patients and payers.
He continues to say that EMRs and health information exchanges have had “limited success in addressing the myriad of nuanced applications and unstructured content outside of core administrative patient records and financial billing processes.”
Holloway proposes that support for multi-disciplinary care and robust, multi-node interoperability will never be achieved without a more holistic approach to integrating structured and unstructured data.
Make the connection, see your whole patient
Providing a “holistic approach” to integrating structured and unstructured healthcare content is a core focus at Hyland Healthcare. Experience has shown that providing a suite of connected healthcare solutions allows healthcare providers to harness the unstructured content in every corner of their enterprise — whether it be a diagnostic medical image, clinical document, video file or audio recording — and link it to the core clinical or business applications they use every day. Addressing unstructured content needs is made possible by combining both a full suite of content services and enterprise imaging tools.
In short, healthcare providers – and by extension the entire healthcare enterprise – work best when it is possible to see your whole patient. By enhancing the EHR or other core clinical application with unstructured content that currently resides in disparate data silos, provider organizations can complete the patient picture. This delivers a truly comprehensive medical information repository at the fingertips of key healthcare stakeholders.
As the addiction epidemic continues to plague even the smallest of communities throughout the country, substance abuse treatment specialists from coast to coast have embarked on a unified effort to raise the tide to improve the continuum of care for individuals struggling to break the cycle.
The national interoperability committee has been making strides over the last year to ensure that regardless of a patient’s unique individual treatment history, care providers are able to efficiently receive seamless access to the complete detailed medical records necessary to begin helping create lasting and effective care.
The committee effort is spearheaded by ZenCharts co-founder Dan Callahan, a 36-year veteran of the behavioral health care industry.
“It’s not uncommon for a patient to go through rehab five or more times — I’ve seen some with over 20 — and communicating information from each of those episodes can be where things start to fall apart,” Callahan said. “Clinicians need the tools to help make the right decisions. If they have all the data, they can see what the patient went through — what was the length of detox? What things were tried, how were they tried and were they were successful?”
With the fragmentation of EHR systems across the country, and privacy laws, sharing medical records can be a significant hangup. When that happens, it puts the burden on the patient to bring a new provider up to speed.
“We’re making changes in the industry as a whole, and helping push the boundaries for how we can help these people,” Callahan said. “We need to help clinicians meet and work with patients where they currently are, and know more accurately where they’ve been.”
By Gevik Nalbandian, vice president of software development, NextGate
Gevik Nalbandian
If you wanted a clear snapshot of the progress we’ve made—or rather, haven’t made—in patient data sharing and exchange, look no further than a new report from the American Hospital Association (AHA) and six other national hospital associations—America’s Essential Hospitals, Association of American Medical Colleges, Catholic Health Association of the United States, Children’s Hospital Association, Federation of American Hospitals and the National Association for Behavioral Healthcare.
Urging all stakeholders to “unite in accelerating interoperability,” the report, released January 22, is a grass roots effort to get hospitals, EHR vendors, consumers, health information exchanges (HIEs), government and medical device companies to come to the table, play their respective roles, and make full interoperability a reality.
The benefits of interoperability are obvious: better care coordination, improved patient safety and care quality, reduced costs, increased efficiencies and the conduit to population health. Interoperability is also increasingly a legal requirement and prerequisite for reimbursement.
So why has healthcare’s goal of industry-wide interoperability remained so elusive?
Errors in prescription can happen for various reasons, like pharmacists’ incompetence, miscommunication between clinicians or doctor’s bad handwriting. Among medication errors, prescription inaccuracy is one of the major causes of concern for healthcare professionals. Today’s most effective technological solution is to implement an electronic prescribing system. With the help of e-prescribing software, prescription errors can be prevented in 80 percent of cases. It is also an actual solution for the opioid epidemic that puts Americans’ lives at risk.
The results, indeed, are impressive. But at the same time, eRx systems are considered inconvenient and costly for small practices. We’ve tried to explore e-prescribing market and identify the main problems of widespread system adoption.
Hitchhiker’s guide to eRx
Electronic prescribing (eRx) is a system that enables healthcare providers to generate digital prescriptions and send them to pharmacies directly from the point of care. e-Prescribing, in fact, improves accuracy, enhances patient safety and quality of care since there is no handwriting.
Systems integrated with EHRs, which include comprehensive patient data.
Stand-alone systems, which means that they can be used only for e-prescribing.
Some eRx systems offer advanced features that allow healthcare providers to access generic medication alternatives, insurance benefit info, and patient medication lists and histories. These extra features have the potential to improve physicians’ decision-making capabilities and increase the use of e-prescribing systems.
E-prescribing market analysis
A prospective EHR vendor has to comply with the regulatory requirements of their customers and know how to develop e-prescribing software. But is investing in eRx worth it?
According to the recent Transparency Market Research, the global market for e-prescribing is expected to reach a CAGR (Compound Annual Growth Rate) of 23.5 percent from 2013 to 2019. Persistent Market Research estimated that the market will reach $887.8 million in 2019.
While Europe holds the largest share in e-prescribing market, the US turned out to be the fastest-growing region. Indeed, increasing adoption of healthcare management software and extensive use of health IT for patient engagement are the key factors in industry growth. Furthermore, electronic prescribing is a requirement for healthcare providers aiming at achieving meaningful use under the Medicare and Medicaid EHR Incentive Programs.
What do prospective vendors need to begin with electronic prescribing?
Major players on e-prescribing market: Cerner Corporation, DrFirst, HealthFusion, Surescripts, Allscripts Healthcare Solutions Inc., Aprima Medical Software, eClinicalWorks, athenahealth Inc. and Relayhealth Corporation.
To show what usability results you can expect, we have chosen the case of Surescript as an “open-source” company. Surescript is a VA-based operator of a nationwide electronic network for prescription-related data and information. Its platform connects EHRs, pharmacy benefit managers (PBMs), pharmacies and clinicians, plus health plans, long-term and post-acute care organizations.
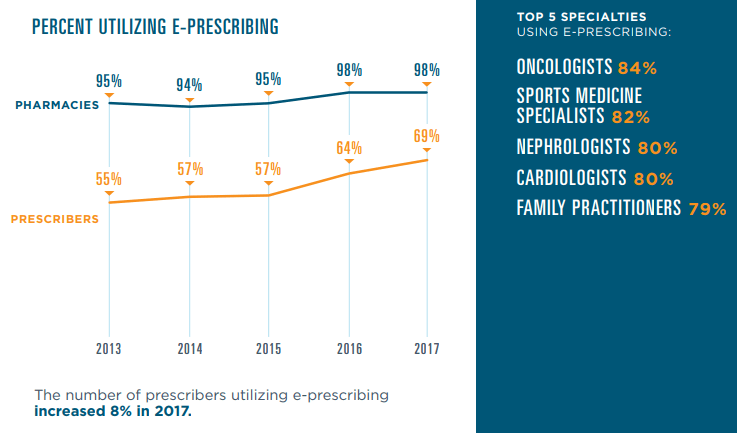
Their 2017 National Progress report shows that 13.7 billion secure health transactions took place via the Surescripts network including 1.74 billio e-prescriptions. This is a 26 percent increase from 2016. This improvement was owing to five key elements: Drug Description, Representative National Drug Code (NDC), RxNorm, Structured and Codified Sig and Potency Unit Code.
Moreover, the network connected 1.47 million healthcare professionals — 13 percent more than in 2016 — with secure patient data for 233 million Americans, or 71 percent of the population.
Various government initiatives which focus on reducing medical errors, and the need to cut escalating healthcare costs foster the growth of the eRx market. The increasing cooperation between software vendors and network providers and the vast untapped regions are expected to provide significant development opportunities for industry players.