The casualty claim arena involves evaluating and payment of claims for claimants who have suffered from an auto accident or workers’ compensation injury. This side of the health payment continuum has been omitted from the Health Insurance Portability and Accountability Act (HIPAA) as a covered entity.
This means that casualty claim insurers are not required to abide by the standards set forth in HIPAA and that these standards only apply to the health payer. Omitting the ICD-10 in casualty claims from standards does have merit, but when it comes to standardization, all health claims should be adjudicated and paid in the same manner. Why should a provider charge differently and be paid differently when the payer of the claim is not on the health side? This is a question many casualty payers ask and not being part of the standardization only raises the question more.
There is no option for submission of claims by the covered entity to not be compliant by October 1, 2014 with the International Classification of Diseases, 10 Revision (ICD-10). Why is it a good idea to omit the casualty payer from these standards if the majority of health payments are made using this new standard? In addition, if providers are covered entities, then why would the casualty payer not speak the same code language? It’s almost like trying to communicate in a foreign country without the benefit of knowing the language.
Over the past year, economic pressure and regulatory changes have increased scrutiny around areas of inefficiency within the healthcare industry. With new policies like the Affordable Care Act creating the need to improve patient outcomes and prevention, 2014 will be the year for much needed efficiency upgrades across the board at hospitals. And with mounting pressure to cut costs amidst anticipated physician and other major shortages, new and innovative ways to leverage technology will be called upon to usher in changes for the healthcare industry.
The business of care will continue to be a major area of focus for hospitals in 2014. Preventable, adverse events because of medical errors cost the healthcare industry more than $29 billion in 2013 and have led to between 50,000 to 100,000 deaths each year. Healthcare professionals and hospitals cannot afford to continue accepting medical errors as balance sheet losses, which are not only jeopardizing profitability, but patient care. To save money and improve patient care at the same time, hospitals will look to learn from technology being used successfully by other industries in 2014 to enhance real-time analysis and, thereby, prevention and outcomes.
PricewaterhouseCoopers released its 2013 third quarter healthcare mergers and acquisitions report and there a small uptick over the first two quarters in the number of healthcare deals with 138 total transactions so far. The value of the deals announced is $15.8 billion, up 35 percent over the second quarter, but 2013 is still behind 2012 with volume down 4.6 percent and value down a whopping 25 percent.
For-profit deals were up, continuing the serge from the second quarter, marked by Tenet Healthcare Corporation’s proposed acquisition of Vanguard Health Systems for $4.3 billion, and the third quarter opened with the announcement of Community Health System’s $3.9 billion offer to purchase Health Management Associates (HMA).
Hospital Deals
During Q3 2013, deal volume and value were up when compared to Q3 2012 with the total volume of hospital transactions increased 59 percent from 12 in Q3 2012 to 19 in Q3 2013. Overall deal value increased significantly from $38 million in Q3 2012 to $12.3 billion in Q3 2013. This is largely the result of two $1+ billion transactions in Q3 2013.
The two $1+ billion transactions announced in Q3 2013 were responsible for the significant increase in total deal value.
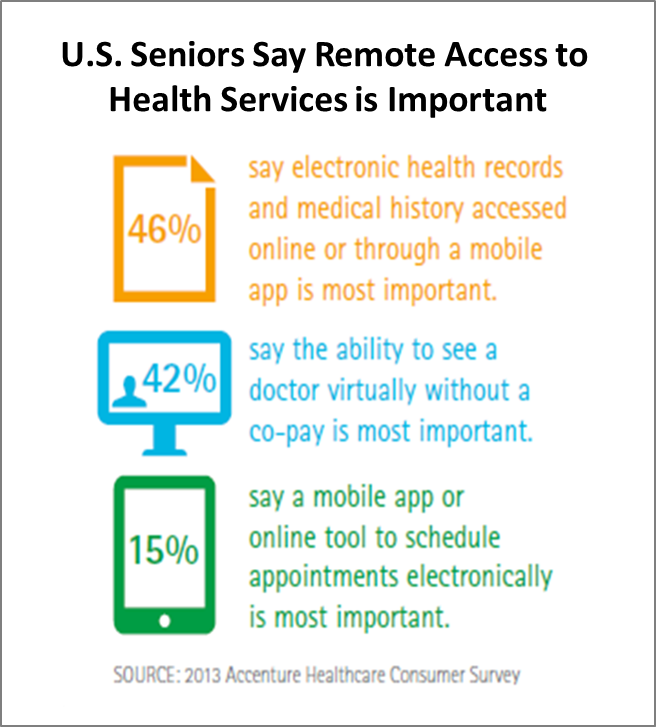
According to a recent Accenture survey, more tech-savvy seniors are seeking digital option for managing their health services remotely. With an estimated 3.5 million U.S. citizens a year expected to reach 65 years-old through 20231, many want access to healthcare technology, such as virtual physician consultations (42 percent) and self-serve tools (62 percent) like online appointment scheduling. Only a third of healthcare providers currently offer such capabilities.
Accenture says that the rising population of seniors are active online. Internet use between 2000 to 2012 tripled for those 65 and older and doubled among those 50 to 64 years old. Accenture says that at least three-fourths of Medicare recipients access the Internet, at least once a day, for email (91 percent) or to conduct online searches (73 percent) and a third access social media sites, such as Facebook, at least once a week.
Two-thirds of seniors (67 percent) surveyed say that access to their health information is important, but only 28 percent currently have full access to their electronic health records. Similarly, 70 percent of those surveyed believe it’s important to be able to request prescription refills electronically, but, fewer than half (46 percent) say they can do so today. And, the majority (58 percent) want to be able to email healthcare providers, but only 15 percent say they currently have that capability.
“Just as seniors are turning to the Internet for banking, shopping, entertainment and communications, they also expect to handle certain aspects of their healthcare services online,” said Jill Dailey, managing director of payer strategy, Accenture Health.
Ohio Republican Senator Rob Portman recently submitted a bill, the Behavioral Health Information Technology Coordination Act, that would add mental health providers to the nation’s EHR network, which essentially has been the catalyst for the surge in adoption of health information technology systems.
Mental health providers are not eligible to receive federal electronic health record incentive payments under the meaningful use program.
According to Portman’s news release on the topic, “Due to a disconnect between our nation’s doctors and mental health care professionals, Americans suffering from mental illness are among the nation’s most underserved and overlooked populations. By fixing an oversight in the system and making health IT the bedrock to fully integrated care, my bill will enhance care and treatment for the mentally ill and put them on a path to lead healthy and productive lives.”
Healthcare organizations maintain a juggling act of caring not only for their patients’ well being, but also the safety and security of the sensitive information that comes in the front door with every patient, doctor, technician and nurse. Data security issues are top-of-mind for information technology professionals in healthcare today, driven by a trifecta of factors: the large number of endpoint devices in use; a rise in the number and frequency of malicious attacks; and strict privacy laws such as HIPAA and regulations related to the Affordable Care Act.
For healthcare IT professionals, it has never been more important to ensure that endpoint security systems are up-to-date and functioning properly so that every endpoint is constantly secure and meeting compliance.
Take HIPAA regulations, which require that end user devices containing sensitive data cannot also have unapproved software running on them. Knowing exactly what software is installed on hundreds or even thousands of endpoints can be tremendously difficult, especially when there isn’t an easy automated way to track this information. Unapproved software is just the tip of the iceberg. What about approved software that isn’t working properly? For example, antivirus software installed on a PC running in a doctor’s office may be outdated, or completely disabled, without the administrator’s knowledge. This gives attackers an open door from this individual endpoint to gain access to the larger network—and a whole host of private information.
Guest post by Ellen Derrico, director of global market development, life sciences and healthcare at QlikTech.
Electronic health records (EHRs) are getting a lot of attention these days, but amid the hype there are skeptics out there arguing that the EHR is old news. However, I’d like to argue that the EHR is not dead; in fact, it’s growing up.
Today’s EHRs are so much more than a digital version of a paper chart. They are evolving and getting more sophisticated. One of the most promising and exciting developments of this is the integration of data discovery and analytics to analyze and compare EHR data. Where business intelligence (BI) was once used primarily to analyze data from a business perspective – revenue cycle management, finance, supply chain management – it’s increasingly being used to analyze patient data, physician performance, facility and utilization – all to improve clinical outcomes.
In healthcare, data discovery and analytics offer the possibility of improving patient care by synchronizing the resource planning with patient logistics and allowing physicians and nurses to focus on improving performance. With BI technology medical practitioners can look across data from different people and locations to support decision making not only for their individual patients, but also for larger patient populations. As a result, practitioners can improve patient outcomes and population health.
Recently, the president of the National Association for Home Care & Hospice (NAHC) called on all American’s to commemorate National Home Care & Hospice Month. He also stated that in the coming years, home health care is poised to play a central role in the delivery of healthcare throughout the country. Yet, the growing home health market is not without challenges. Solutions that blend innovation and mobility at the point of care can help pave the way for strong patient-caregiver interactions and support positive outcomes.
Home Health Poses Challenges: Mobile Solutions Can Improve Care Delivery
An aging population and tough new compliance and regulatory issues are posing challenges for the home healthcare segment. The unique and specific needs of the home healthcare market must play a paramount role in organizations seeking to develop mobile solutions to address these issues. Home caregivers urgently need “smart” solutions that address not only patient privacy, but also, wireless connectivity, mobile printing, security and remote data access.
There are a number of issues and trends impacting the healthcare industry that solution providers and caregivers need to keep top-of-mind:
Reimbursements/Re-admissions – Medicare reimbursement reductions and new penalties are being imposed on hospitals with high avoidable re-admissions. This increases the pressure on home health agencies to leverage technology to aid patients in following aftercare instructions, adhering to medication plans and accessing their medical information – all to better prevent costly re-admissions from occurring.