By Joe Polaris, senior vice president of product and technology, R1 RCM.
Joe Polaris
This year promises many new opportunities to apply technology to improve the healthcare revenue cycle. The recent HIMSS conference, for instance, featured many exciting use cases for machine learning and artificial intelligence (AI). However, before rushing to implement any of the latest solutions, let’s step back for a moment.
While there is plenty of emerging revenue cycle technology, there is also still a fair amount of complexity when it comes to implementing these capabilities. Most organizations typically have a significant amount of disorganization to deal with on the back end of their billing processes, as well as disparate technology systems that don’t work together. Many organizational leaders also are growing tired of only achieving incremental improvements to the revenue cycle through stand-alone revenue cycle management (RCM) technology, especially with rising total administrative costs and cost to collect.
That means we simply cannot afford to implement “quick-fix” RCM technologies that fail to support future goals. In an industry known for emphasizing quarter-by-quarter financials, we must begin taking a longer view. Rather than trying to establish 2019 implementation priorities, think about using the rest of 2019 to set the foundation for a holistic RCM transformation.
Perhaps the question to ask this year is: “Where do we want to be in three years – in terms of process efficiency, cash flow and an experience that delights our patients?”
Map RCM to the patient journey
Answering that question requires a holistic assessment of the entire revenue cycle, especially as it relates to the patient journey. Although that’s not a small undertaking, it allows healthcare organizations to build a thoughtful, realistic roadmap for long-term RCM transformation. In turn, such planning helps organizations realize greater value from all their RCM technology investments. Consider these four steps:
Evaluate: Although some healthcare organizations are further along when it comes to more efficient and patient-centered RCM, most are just starting to explore due to a wide variety of situational limitations. Escaping such constraints will require you to map out the entire patient journey end-to-end. Then, look at the map to identify areas of potential revenue cycle satisfaction for patients, as well as their most significant pain points.
Plan: After evaluating your RCM strengths and weaknesses, prioritize those processes in which technology has the greatest potential to remove waste, create capacity or give back operational expense. When deciding which solutions to implement, remember to take a broader, longer-term focus. Your organization should avoid the temptation of “quick wins” and instead focus on a viable long-term path that will meet your holistic, collective objectives. By generating a long-term plan, you will also incrementally create business value and move toward a more well-defined end-state vision. The most impactful digital transformation might come from phasing in the adoption of a comprehensive platform, as well as combining digital self-service technology and other automation capabilities — some of which may take hold quickly, while others may require more time.
By Paurakh Rajbhandary, senior biomedical engineer, VitalConnect.
Paurakh Rajbhandary
The need for hospitals and physicians to recognize and react to patients showing early signs and symptoms of clinical deterioration has resulted in the creation of a rapid response system (RRS). Patient deterioration prior to adverse events including cardiac arrest and ICU admission has been reported with hemodynamic antecedents in 60 percent of critical events. For example, patients who develop cardiopulmonary arrests exhibit clinical deterioration such as respiratory distress as early as eight hours in advance of arrest in 84 percent of the patients.
The RRS system, aimed at detecting precursors to and reducing such avoidable adverse events, comprises of track-and-trigger or afferent (detection) component for event detection, and efferent (response) component comprising of rapid response team (RRT) or medical emergency team for intervention and prevention of patient deterioration. Rapid response systems also comprises of administrative components and continual process improvement.
MET criteria is commonly used as an afferent triggering metric currently in many healthcare systems, but MET criteria is based on threshold of single vital or physiological measurement. The need of a good afferent component to RRS has been previously pointed out. Early warning score (EWS) combines multiple vital measurements to create a more comprehensive yet simple unified score that has been clinically validated to indicate increased risk of patient deterioration.
Among several different versions of early warning scores currently used in different healthcare settings, National Early Warning Score (NEWS) is standardized and endorsed by National Health Services (NHS) and Royal College of Physicians (RCP) in an effort to eliminate lack of consistency in the clinical workflow.
NEWS is an aggregate score calculated based on six physiological parameters: respiratory rate, oxygen saturations, temperature, systolic blood pressure, pulse rate, level of consciousness, and whether the patient is using supplemental oxygen. A sub-score within from zero to three is allocated to each of these parameters, giving an aggregated NEWS score between zero and 20 reflecting how patient status varies from the norm. The sub-score contribution criteria for each of the parameters has been determined and validated clinically by the NHS and Royal College of Physicians. The NEWS score dictates clinical urgency, the magnitude of response as well as frequency of clinical monitoring of the patient.
NEWS has demonstrated superior performance in determining patients at risk of cardiac arrest, unanticipated intensive care unit (ICU) admission or death within 24 hours of a NEWS value compared to 33 other early warning scores. Sensitivity and specificity performance of early warning scores dictates the trade off between alarm fatigue and ability to flag all deteriorating patients. Studies have shown that NEWS provides the best compromise between sensitivity and specificity allowing hospitals and healthcare providers to predict and reduce the aforementioned deterioration and improve patient outcome.
National Health Service (NHS) has been pushing to implement NEWS in all of its hospitals since its initial launch in 2012, having achieved implementation at 70 percent of acute trusts in England and with other forms of early warning scores in the remaining trusts. Variation in early warning scores systems can lead to confusion and potentially compromise performance of the detection of patient deterioration, patient safety and positive outcome. With this in mind, NHS are launching a campaign to increase NEWS use to 100 percent at acute and ambulance settings by March 2019.
The statistics related to chronic disease management are staggering. According to the US National Center for Health Statistics, 40 percent of the US population have chronic conditions and almost one-third of this patient population has multiple chronic conditions. It’s a struggle to manage and engage these patients and keep the “sickest of the sick” at home, receiving care, vs. returning to the hospital or another facility. These high-risk members are also the most expensive. The treatment of patients with chronic conditions accounts for three-quarters of the $2.2 trillion in healthcare spending, with roughly 96 cents per dollar spent in Medicare and 83 cents per dollar in Medicaid, according to the CDC.
Unfortunately, these patients may be “frequent fliers” in a health system; they typically need more attention between care appointments and often rely on emergency medical services and/or the emergency room to answer questions and provide care in non-critical situations. Significant opportunities exist for technology and touchpoints to bring ongoing care and support closer to these patients. Virtual care technology can improve care coordination and increase patient access to convenient care 24/7. Frequent touchpoints can continually engage chronic care patients, resulting in better disease management, improved outcomes and reduced costs.
Post-acute care organizations are embracing the use of a virtual care communication platform to engage chronic care patients and optimize their agency’s available resources. Using a combination of a video-based platform and readily available smartphones, tablets and PCs, home health clinicians can quickly connect, communicate and collaborate with patients – and colleagues — to ensure patients are actively monitored and motivated in their care without a series of in-home visits.
Ongoing messages and a series of virtual visits can augment – and even replace – many traditional in-person visits, effectively reducing the costs and liabilities associated with nurses driving to each patient’s home. The virtual visit can also include a clinician, a pharmacist and even an interpreter, depending on the patient’s needs. During virtual visits, home health providers can use video to detect potential patient issues before an in-person consult is needed and deliver preventive care during the call, minimizing the need for an immediate in-person intervention.
Over the last few decades, we have seen exponential growth in technology. Hardware and software permeate the world around us. The world has become a smaller place with distances presenting less of an obstacle. Businesses manage employees across the globe with remote collaboration software. We see advanced satellites going into space, mapping the unknown. We know much more about geology thanks to sophisticated equipment.
Technology is evolving very fast, and so is the health sector. However, the impact of technology has been most profound in the field of medicine. This blog discusses how.
Technology in the health sector
Technology has played an important role in improving healthcare. We have advanced treatments and procedures that seem commonplace today. The improvement itself has been constant. You can see it from the invention of X-rays to precise surgical procedures. These advancements have made it possible for humans to live healthier lives. They have resulted in a longer average life expectancy. As we go into the 21st Century, there is no reason to suppose that technology is slowing this process down. The most recent example is medical science developing a promising AIDS treatment. Technology and science help cure diseases and improve the quality of our lives even more. Here are only four ways in which technology is improving the health sector:
Gene sequencing
Wearable medical devices
Remote medical monitoring
Digital medical records
Let’s take a closer look at how technology impacts these specific areas in the health sector.
Gene sequencing
Human genomics has earned a reputation as the future of medical science. What gene sequencing refers to is sequencing and analyzing a person’s genome. This information also goes to the person. Sequencing the human genome is one of humanity’s biggest achievements. Especially in the last four decades. The human genome is like an instruction manual for the human body. It may help people detect and avert hereditary diseases and live a better life.
Recent research was published by the Washington Post about malware that was created to disrupt medical imaging equipment and networks. This is yet another wake-up call for the healthcare industry that been underinvesting in security for the last decade. Quite simply, there is a misconception that hospitals’ internal networks are a safe harbor from external cyberattacks. This is despite the fact that the real-world data has repeatedly shown that healthcare is one of the top industries under attack for the last five years. While previous attacks mainly focused on stealing personal health information, this research demonstrates how serious or even deadly an attack to healthcare can be.
There are a few reasons why cyberattacks in healthcare today can have devastating consequences.
Medical device vulnerabilities
Many medical devices inside hospitals are running decade old operating systems and applications that have many well-known vulnerabilities. In fact, it may be a surprise to many that the vast majority of imaging systems run on Windows OS. Further, recent Zingbox research shows that today, 1 out of 4 imaging systems run on OSes that are no longer supported. By next year, 85% of imaging systems are expected to run on End-of-Lifed OSes as Microsoft terminates support for some of their popular Windows OSes.
To make matters worse, most medical device manufacturers lack strong in-house cybersecurity expertise. While their expertise lies in device reliability and accuracy, which continue to be top requirements for connected medical devices, the lack of cybersecurity expertise puts the device reliability and accuracy into question. The lack of cyber-specific expertise also limits manufacturers’ ability to “bake in” cybersecurity measures on the device.
One might think that patches and upgrades are the answer. Unfortunately, no. FDA certification and other requirements pose significant hurdles for manufacturers to apply patches or upgrades to devices already deployed at hospitals.
Tools designed for IoT
Many hospitals lack the tools to monitor life-critical devices with 100% assurance of uninterrupted service and care. Such tools must be completely transparent to the device and in no way interfere or hamper its operation. Yet, organizations continue to rely on traditional IT security solutions for IoT. Such network security tools like firewalls and antiviruses result in security gaps that hackers can easily exploit.
Vulnerabilities that stem from inadequate IoT security tools:
Most network security solutions often cannot discern a PC from a CT scanner, whereas such a distinction is critical for cybersecurity.
CT scanner’s communication is almost never encrypted, device access doesn’t require basic authentication, and given the mobility of typical CT scanners, the devices can be connected to any internal network, according to Zingbox’s research findings.
Connecting a device to any network breaks the basic micro-segmentation policies IT teams have been encouraged to deploy for cybersecurity.
Today, the Trump Administration proposed changes to further the agency’s priority to transform the healthcare delivery system through competition and innovation while providing patients with better value and results. The proposed rule would update Medicare payment policies for hospitals under the Inpatient Prospective Payment System (IPPS) and the Long-Term Care Hospital (LTCH) Prospective Payment System (PPS) for fiscal year 2020 and advances two key CMS priorities, “Rethinking Rural Health” and “Unleashing Innovation,” by proposing historic changes to the way Medicare pays hospitals.
“One in five Americans are living in rural areas and the hospitals that serve them are the backbone of our nation’s healthcare system,” said CMS Administrator Seema Verma. “Rural Americans face many obstacles as the result of our fragmented healthcare system, including living in communities with disproportionally higher poverty rates, more chronic conditions, and more uninsured or under insured individuals. The Trump Administration is committed to addressing inequities in healthcare, which is why we are proposing historic Medicare payment changes that will help bring stability to rural hospitals and improve patients’ access to quality healthcare.”
The inpatient hospital wage index specifies how inpatient payment rates are adjusted to account for local differences in wages that hospitals face in their respective labor markets. It is intended to measure differences in hospital wage rates across geographic regions and is updated annually based on wage data reported by hospitals. Hospitals located in areas with wages less than the national average receive a lower Medicare payment rate than hospitals located in areas with wages higher than the national average. For example, a hospital in a rural community could receive a Medicare payment of about $4,000 for treating a beneficiary admitted for pneumonia while a hospital in a high wage area (like many urban communities) could receive a Medicare payment of nearly $6,000 for the same case, due to differences in their wage index.
In last year’s proposed rule, CMS invited comments on changes to the Medicare inpatient hospital wage index. Many responses reflected a common concern that the current wage index system makes the disparities between high and low wage index hospitals worse. High wage index hospitals, by virtue of higher Medicare payments, can afford to pay their staff more, allowing the hospitals to continue operating as high wage index hospitals. Conversely, low wage index hospitals often cannot afford to pay wages that would allow them to climb to a higher wage index. Over time, this creates a downward spiral that increases the disparity in payments between high wage index hospitals and low wage index hospitals, and payment for rural hospitals and other low wage index hospitals declines.
To address these disparities, CMS is proposing to increase the wage index of low wage index hospitals. This change would ensure that people living in rural areas have access to high quality, affordable healthcare. CMS is considering several ways to implement this change, and the agency looks forward to comments on the different approaches.
The Trump Administration is also announcing proposals that would ensure Medicare beneficiaries have access to a world-class healthcare system by unleashing innovation in medical technology and removing potential barriers to innovation and competition in order to expedite access to novel medical technology.
“Transformative technologies are coming to the private market, but Medicare’s antiquated payment systems have not contemplated these technologies,” said Verma. “I am particularly concerned about cases that have been reported to the agency in which Medicare’s inadequate payment has led hospitals to curtail access to needed therapies. We must continually update our policies in response to the rapid pace of advancement in medical science.”
U.S. Department of Health and Human Services (HHS) Secretary Alex Azar and Centers for Medicare & Medicaid Services (CMS) Administrator Seema Verma announce the CMS Primary Cares Initiative, a new set of payment models that will transform primary care to deliver better value for patients throughout the healthcare system. The CMS Primary Cares Initiative will aim to reduce administrative burdens and empower primary care providers to spend more time caring for patients while reducing overall healthcare costs, HHS said in a statement.
Alex Azar
“For years, policymakers have talked about building an American healthcare system that focuses on primary care, pays for value, and places the patient at the center. These new models represent the biggest step ever taken toward that vision,” said HHS Secretary Alex Azar. “Building on the experience of previous models and ideas of past administrations, these models will test out paying for health and outcomes rather than procedures on a much larger scale than ever before. These models can serve as an inflection point for value-based transformation of our healthcare system, and American patients and providers will be the first ones to benefit.”
Empirical evidence shows that strengthening primary care is associated with higher quality, better outcomes, and lower costs within and across major population subgroups. Despite this evidence, primary care spending accounts for a small portion of total cost of care, and is even lower for patients with complex, chronic conditions, HHS said.
CMS’s experience with innovative models, programs and demonstrations to date have shown that when incentives for primary care clinicians are aligned to reward the provision of high-value care, the quality and cost effectiveness of patient care improves, the organization cited.
Seema Verma
“As we seek to unleash innovation in our health care system, we recognize that the road to value must have as many lanes as possible,” said CMS Administrator Seema Verma. “Our Primary Cares Initiative is designed to give clinicians different options that advance our goal to deliver better care at a lower cost while allowing clinicians to focus on what they do best: treating patients.”
Administered through the CMS Innovation Center, the CMS Primary Cares Initiative will provide primary care practices and other providers with five new payment model options under two paths:
Primary Care First and Direct Contracting.
The five payment model options are:
Primary Care First (PCF)
Primary Care First – High Need Populations
Direct Contracting – Global
Direct Contracting – Professional
Direct Contracting – Geographic
The Primary Care First (PCF) payment model options will test whether financial risk and performance based payments that reward primary care practitioners and other clinicians for easily understood, actionable outcomes will reduce total Medicare expenditures, preserve or enhance quality of care, and improve patient health outcomes. PCF will provide payment to practices through a simplified total monthly payment that allows clinicians to focus on caring for patients rather than their revenue cycle. PCF also includes a payment model option that provides higher payments to practices that specialize in care for high need patients, including those with complex, chronic needs and seriously ill populations (SIP).
Both models under PCF incentivize providers to reduce hospital utilization and total cost of care by potentially significantly rewarding them through performance-based payment adjustments based on their performance. These models seek to improve quality of care, specifically patients’ experiences of care and key outcome-based clinical quality measures, which may include controlling high blood pressure, managing diabetes mellitus and screening for colorectal cancer. PCF will be tested for five years and is scheduled to begin in January 2020. A second application round is also planned for participants starting in January 2021.
By Chris Jaeger, head of ACO and health system strategy, AristaMD.
Rural hospitals are facing severe challenges in maintaining operating margin, with uncompensated care being a major factor. Telehealth eConsult platform use in local primary care settings to improve “right time, right place, right provider care” have been shown to decrease the number of patients receiving avoidable and unnecessary care within the hospital setting, thus supporting hospital’s ability to mitigate uncompensated care.
Uncompensated care is an overall measure of hospital care provided for which payment was not received from the patient or payer group. It equates to the sum of a hospital’s bad debt — the financial assistance it provides. Financial assistance includes care for which hospitals never expected to be reimbursed and care provided at a reduced cost for those in need. A hospital incurs bad debt when it cannot obtain re-imbursement for care provided; this happens when patients are unable to pay their bills, but do not apply for financial assistance, or are unwilling to pay their bills.
Hospitals, both nonprofit and for-profit, provide uncompensated care for individuals who are uninsured and under insured.
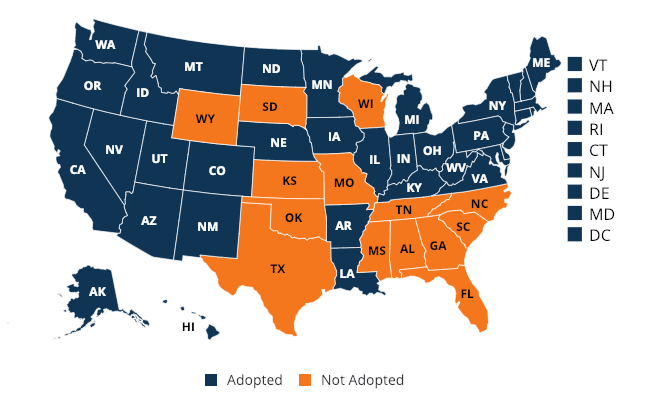
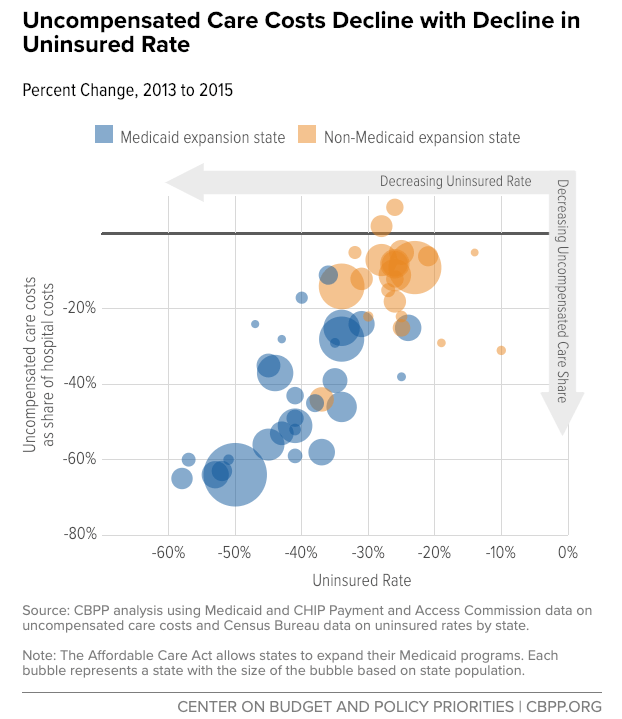
Though there has been a noted decline in uncompensated care since the 2014 passage of the Affordable Care Act and Medicaid expansion, this has not carried over to states not part of the expansion. States that expanded Medicaid to low-income adults under the ACA recognized a 47 percent decrease in uncompensated care costs, on average, compared to an 11 percent decrease in states that did not expand Medicaid.
(Coverage map as of Feb 2019)
Uncompensated care and dropping revenue margins are causing hospitals, especially in rural areas, to close. “While Medicaid expansion has improved all hospitals’ operating margins and total margins, the effect was particularly pronounced in rural areas,” noted a report from the Center on Budget and Policy Priorities. A recent study by the North Carolina Rural Health Research Program (NC-RHRP) at the University of North Carolina Cecil G. Sheps Center for Health Services Research (UNC-CH) showed that since 2010, 89 rural hospitals in 26 states have closed.
Much of this uncompensated care could be prevented through primary care intervention. A report, released by Premier, found that six common chronic conditions accounted for 60 percent of 24 million Emergency Department (ED) visits in 2017; out of that 60 percent, approximately one third of the visits (4.3 million) were likely preventable and could be treated in a less expensive outpatient setting.





 “One in five Americans are living in rural areas and the hospitals that serve them are the backbone of our nation’s healthcare system,” said CMS Administrator Seema Verma. “Rural Americans face many obstacles as the result of our fragmented healthcare system, including living in communities with disproportionally higher poverty rates, more chronic conditions, and more uninsured or under insured individuals. The Trump Administration is committed to addressing inequities in healthcare, which is why we are proposing historic Medicare payment changes that will help bring stability to rural hospitals and improve patients’ access to quality healthcare.”
“One in five Americans are living in rural areas and the hospitals that serve them are the backbone of our nation’s healthcare system,” said CMS Administrator Seema Verma. “Rural Americans face many obstacles as the result of our fragmented healthcare system, including living in communities with disproportionally higher poverty rates, more chronic conditions, and more uninsured or under insured individuals. The Trump Administration is committed to addressing inequities in healthcare, which is why we are proposing historic Medicare payment changes that will help bring stability to rural hospitals and improve patients’ access to quality healthcare.”