By Brian Carter, senior vice president of product, Validic.
Brian Carter
Clinicians, CIOs and virtually every person in a decision-making position in a health system is courted multiple times a week by third-party solution developers with amazing products to help them with some of their most pressing problems. The features look great, but at some point they have to ask: does it integrate with my existing clinical workflows in a way that makes it easy to use, hard to forget about, and actually save my team some time?
This question is extremely important; according to one study about clinical decision support (CDS), zero CDS interventions succeeded when they weren’t delivered automatically in the clinician workflow. By contrast, the same study showed that 75 percent of those interventions succeeded when they were automatically presented in clinical workflow. Workflow integration comes in a variety of flavors, with the value of that integration typically (and somewhat unfortunately) proportional to the amount of investment made in preparing for that integration.
Visual integration is the lightest-weight kind of integration. iFrames, SMART apps and “widgets” are all common technologies that come to mind when describing visual integration. Essentially, you are taking one application and layering it as a self-contained component inside another application. This ideally includes a single sign-on function so the person signed into the main application doesn’t have to sign into another widget on their screen.
A common example on the web is Disqus. If you scroll to the comments section of a web page to share your opinions, you’ll find a nicely-embedded component with other people’s comments. But, if you want to contribute a comment yourself, you have to sign in. This comment feature is actually a totally different application provided by another company called Disqus, which was visually integrated with a few lines of code.
Data integration is often what’s being talked about when interoperability comes up. Data integration simply means enabling the data from one application to flow meaningfully into another application. The concept is simple, but the application of this strategy can be highly complex. It involves getting two systems to not only get data from one place to another, but also to be formatted and codified in a way that the receiving system can actually understand it.
Technologies common in health care surrounding data integration include the emerging FHIR specification from HL7, legacy APIs provided by EHR vendors, health information exchanges that serve as intermediaries between different systems, as well as enterprise data warehouses and big data platforms. Data integration is a critical strategy whenever users of one system need information that users of another system have generated.
By Susan DeCathelineau, vice president of global healthcare sales and services, Hyland Healthcare.
Susan DeCathelineau
Healthcare interoperability continues to be a critical topic facing healthcare technology leaders. There’s no question that achieving true healthcare interoperability is key to moving the industry forward by enabling the type of information exchange that can streamline workflows, inform clinical decision making and enable precision medicine.
However, much of the current interoperability discussion is focused on ensuring core systems, i.e. Electronic Medical Records (EMRs) are compatible with one another. Yet there is one issue that is largely overlooked: the crucial role of integrating structured data with unstructured patient information.
For example, EMRs are designed to capture and manage structured patient data, and they do that job well. That is to say, they capture content using controlled vocabulary rather than narrative text. But the lack of structured data and standardization in the healthcare industry today creates major issues when sharing EMR content within and across healthcare organizations.
EMRs are not built to natively ingest the plethora of unstructured information that exists on a patient. This unstructured content includes things like diagnostic medical images, clinical documents and notes, visible light images and more. According to many industry estimates, as much as 75 percent of the information that exists on a patient lives outside of core applications like EHRs. Instead, this unstructured content is scattered in a multitude of legacy data silos.
Manage your unstructured clinical content
A recent whitepaper by Signify Research illustrates just how pervasive ineffective management of unstructured content is in today’s health systems, and just how vital this effort is to interoperability initiatives. In the paper, author Steve Holloway explains how the growth of healthcare networks resulting from merger and consolidation activity is driving the need for true interoperability. These ever-larger healthcare enterprises are increasing demand for incoming and outgoing information exchange between a diverse ecosystem of providers, patients and payers.
He continues to say that EMRs and health information exchanges have had “limited success in addressing the myriad of nuanced applications and unstructured content outside of core administrative patient records and financial billing processes.”
Holloway proposes that support for multi-disciplinary care and robust, multi-node interoperability will never be achieved without a more holistic approach to integrating structured and unstructured data.
Make the connection, see your whole patient
Providing a “holistic approach” to integrating structured and unstructured healthcare content is a core focus at Hyland Healthcare. Experience has shown that providing a suite of connected healthcare solutions allows healthcare providers to harness the unstructured content in every corner of their enterprise — whether it be a diagnostic medical image, clinical document, video file or audio recording — and link it to the core clinical or business applications they use every day. Addressing unstructured content needs is made possible by combining both a full suite of content services and enterprise imaging tools.
In short, healthcare providers – and by extension the entire healthcare enterprise – work best when it is possible to see your whole patient. By enhancing the EHR or other core clinical application with unstructured content that currently resides in disparate data silos, provider organizations can complete the patient picture. This delivers a truly comprehensive medical information repository at the fingertips of key healthcare stakeholders.
Sudden cardiac arrest (SCA) remains the leading cause of death in athletes, with recent studies showing the condition occurs more frequently than historical estimates.[1] Currently, there are more than 350,000 SCA-related deaths each year.[2] Stuart Long, CEO of InfoBionic, a digital health company that created the MoMe Kardia Platform, confirms that remote cardiac monitoring that is FDA cleared for diagnosis of arrhythmias is the next logical step after an alert from an athletes’ consumer wearable if confirmed by a physician.
Stuart Long
According to a recent study by the University of Toronto, health screenings only identify young athletes who are at risk for cardiac arrest. However, more than 80 percent of cardiac cases are not discovered through systematic screening, researchers say. In fact, a significant problem with current screenings is that they exclude people whom are perceived healthy enough to safely engage in sports.3
A separate study sponsored by the National Institute for Health of 2,640 competitive soccer players featured data collected from 1974 until April 2004. From this population, there were 62 reported cardiac arrests; 24 were sudden death events; and 38 were resuscitated from cardiac arrest.4 SCA is responsible for as many as 20 percent of all deaths in the U.S., according to the study, and “50 percent of sudden cardiac deaths are first cardiac events, meaning the patient did not know they had heart disease,” Dr. Robert J. Myerburg, a professor at the University of Miami (Fla.) and a cardiologist said.5
In the U.S., on average, one young competitive athlete dies suddenly every three days. Young athletes are twice as likely to experience SCA than young non-athletes. Exacerbating the issue is that no two heart conditions are the same, as demonstrated by several young professional athletes who have suffered in-competition cardiac events.6,7
Consumer wearable devices can detect worrisome irregular heartbeat in many cases. However, the perceived lack of accuracy is leading to skepticism around false positives. For example, devices that employ electrocardiogram-like technology can be hindered when an athlete’s skin is wet, limiting or impairing the device’s readout, especially impacted by artifact or noise during intense activity. Wearers who receive an alert through the watch’s technology are instructed to consult a physician who can provide further diagnostics.8
An effective advertising and marketing plan for the head and neck surgeon can capitalize your diverse capabilities. Head and neck surgeon needs successful marketing strategies while strengthening and building their practice. With advertising and marketing, you can get the advantage of a widespread opportunity spectrum. The head and neck surgeons deal with disorders of tongue, jaw, neck, thyroid, parathyroid glands, throat/tonsils, salivary glands, oral cavity and face.
NextGenOMS.com – head and neck surgeon suggests working with an experienced surgeon for diagnostic and preventive care. A surgeon needs extensive training, clinical experience, and knowledge to treat a complex and simple oral cavity, throat, facial, pathologies and head and neck disorders. Along with your practice, you should promote your services to get new patients. Here are some marketing strategies that can help you in this field.
Consistent branding
Do you think your expertise set you apart from others? Without promotion, it can be challenging to spread the news of your expertise. You have to figure out your brand and its uniqueness. Promote it on social media and design your clinic’s website. Facebook may help you to stay in touch with new and old patients.
It is essential to understand the marketing interpretations associated with patients. You must have a deep understanding of the requirements of target patients and answer them appropriately. Understand that you must have a connected relationship with patients to increase their satisfaction.
If your organization handles protected health information (PHI) or electronic Protected Health Information (ePHI), you should be well aware of the Healthcare Insurance Portability and Accountability Act known commonly as HIPAA. The HIPAA compliance is regulated by the federal government and failure to comply with it can attract penalties. Additionally, non-compliance may have severe consequences!
What are the penalties for HIPAA non-compliance?
Congress enacted HIPAA in 1996 with the primary intention of safeguarding sensitive information as people switched jobs. Additionally, the United States’ Department of Health and Human Services (HSS) established HIPAA Privacy Rule in 2003.
The privacy rule defines PHI as any information handled by a covered entity that concerns the health, treatment, or payment information associated with an individual. As technology related crimes increased, HIPAA focused on ePHI where they created three safeguards in 2005. They include:
Administrative safeguards concentrate on all the policies and procedures that demonstrate protection of ePHI by a given entity
Physical safeguards which revolve around controls instituted to limit access to ePHI storage devices
Technical safeguards which focused on safeguarding all the communication channels used to transmit ePHI over open networks
Definition of covered entities and business associates
According to HIPAA, covered entities are all the bodies that are involved in the handling of a patient’s data. They include healthcare providers such as clinicians, doctors, nurses, pharmacists, dentists, and chiropractors as well as all healthcare plans providers such as the HMOs, health assurance entities, and government programs.
HIPAA also considers all healthcare clearinghouses as covered entities that should comply with its regulations. These bodies process nonstandard health-data that they obtain from the covered entities to transform it into standard data.
Business associates are all the institutions that can access the PHI or ePHI since they are contracted by the covered entities to execute specific activities on their behalf. HIPAA demands that your organization have a written contract that elaborates the responsibility of the business associates in upholding the integrity and confidentiality of the PHI that they handle.
Governing of HIPAA
The privacy and security regulations by HIPAA are enforced by the Office for Civil Rights (OCR) which serves under the Department of Health and Human Services (HSS). OCR provides a platform where you can air your complaints against covered entities as well as their business associates. If you feel that there is a data breach, you should visit the OCR website and submit your claims there for evaluation. Alternatively, you can use their portal, mail, fax, or email services.
With hundreds of thousands of clinical trials currently underway worldwide, we are continuously seeing innovation applied to how we treat and cure diseases, but the traditional four-phase method of getting there has not been updated since 1963. What makes this antiquated process for pharmaceutical companies and long wait time for patients in need worth it is the promise of a safe and effective therapy for the vast majority of patients.
This promise, however, is negated before the clinical trial begins when pharmaceutical companies opt to perpetuate the creation of blockbuster treatments for the “average” patient that disregards individual patient disease biology.
The cost of ineffective treatment for both patients and the healthcare industry is high in many ways, and there is a clear need to change the process to bring more effective treatments to market. The current system was developed to provide blanket treatments for a particular disease without considering the disease biology of individuals. Moving forward, pharmaceutical companies first need to study the individual’s disease and then create a personalized treatment for patient subgroups within each therapeutic area.
Precision medicine technology holds the key to meet this need and could change the current clinical trial system that has been in place for years. Companies are working on technology such as this to enable more targeted trials that are smaller, nimbler, equally as effective and safe, and encourage the creation of personalized treatments to finally break the cycle of expensive, ineffective blanket treatments.
Enabling smaller, more effective and affordable trials
For years, patients and doctors have started to become exasperated with this traditional, slow-moving clinical trial model and are searching for a more personalized route as an alternative. Precision medicine offers the unique ability to deeply understand the genetic makeup of patients’ diseases, which in turn would enable the development of better drugs with clinical trials that consist of sample sizes based on genetic disease make-up rather than phenotypic expressions.
Backed by preliminary research into the patients being treated, these smaller and more targeted trials can hypothetically be conducted more rapidly and at lower costs, allowing for breakthrough therapies to come to market faster at potentially more affordable prices.
A key element in achieving end-to-end revenue cycle success in any healthcare operation is proper dedication and maintenance of workflow tools, and those systems that support processes that help organizations meet net revenue expectations.
Workflow optimization and the deployment of tools should be viewed from four perspectives: People, process, technology and metrics/KPIs/reporting.
It is incumbent on healthcare organizations to explore each of these areas related to RCM workflow optimization and consider relevant questions before deploying a fresh approach to workflow processes and automation. First, they must recognize that a balance of concentration of these four components is needed when building operational effectiveness and for the success of workflow strategy, tools and support systems. Furthermore, it is critical for RCM workflows (front, middle and backend) to reflect the uniqueness (location, size, demographics, payer mix, etc.) of the organization.
While there are many benchmarks and strategies in the industry that an organization can follow, adapt to or adopt, the specific characteristics of the organization – whether it’s a rural versus urban facility, the size and makeup of its staff, budgets, effects of recent mergers and acquisitions, and more – must be inputs when building and maintaining effective workflow controls. Principally, dedication to establishing optimization in workflows within revenue cycle operations is a direct result of senior management’s objectives of lowering or maintaining organizational metrics involving departmental and organizational “cost to collect”.
Organizations’ achievement of desired “cost to collect” results comes from their empowerment of senior and middle management and line staff, adoption of sound strategies that are understood and embraced, provision of user-friendly processes and effective deployment of technology – as well as maintenance of technology in a manner that is adaptable and flexible to the user and the organization.
More importantly and in support the first three components, organizations pursuing workflow optimization must have a process in place for measuring and gauging the success of established RCM goals, as well as clear metrics. Metrics are where the rubber meets the road – they’re how organizations know whether the people, process and technology components are functioning efficiently and as intended.
As in any situation where there is a desire to get from one point to another effectively and efficiently, a sound understanding of how metrics support organizational expectations will inform the direction and strategy. It is also important to note that RCM workflow optimization is system agnostic. While each organization has different approaches to workflow support and automation, they need to look at this component relative to the system they have deployed as well as their own uniqueness.
With a dedicated, all-encompassing approach to workflow operations, organizations are better positioned to process patient access, improve eligibility/benefits verification administration processing, improve Point-of-Service (POS) collections, effectively manage claims loads, process appeals in a more timely manner and improve self-pay production and collections. They can also maintain proper coding requirements, improve overall processing, and possibly reduce denials or denial rates, all while improving overall aspects of the revenue cycle continuum to achieve organizational strategic and revenue goals.
While there is no off-the-shelf, cookie-cutter formula to deploy to achieve expected net revenues and RCM optimization, establishing and maintaining benchmarks consistent with the uniqueness of an organization is key to success.
Organizations must address many questions to understand whether workflow operations and technology are hitting the mark. While a holistic approach taking into account people, processes, technology, and metrics is fundamental for true system effectiveness and performance optimization, there are many considerations associated with each of these areas.
People/Resources:
Does your staff have the capacity to perform production requirements needed for organizational success? Additionally, in deploying resources, are team members in the right positions? Are there leaders who can enable others’ success?
Do all RCM staff fully understand their roles relative to the RCM end-to-end continuum? Are staff interchangeable or cross-trained to increase operational understanding or in preparation to fill unexpected gaps?
Does RCM management deploy outsource resources as a stopgap measure?
Are teams looking at “root cause” issues that will affect workflow production goals and objectives?
Processes
In the case of new RCM systems and upgrades to present systems, are workflow processes reviewed or challenged with respect to potential changes in technology?
Are RCM operational workflow processes interchangeable so that any new introducing effects do not create abnormalities, gaps, and workarounds?
Does the organization embrace outsourced help in achieving best practices in workflow processes?
Should the organization consider a central billing office if one does not exist?
While there are more questions organizations ought to consider in reviewing – and correcting – the effectiveness of the RCM continuum, the areas of people and process should guide the use of resources in the most efficient and effective manner. Furthermore, the structure of operations should allow for adaptable departments(s) and an environment that promotes the achievement of organizational goals and the ability to manage expected and unexpected changes.
By Abhinav Shashank, president and co-founder, Innovaccer.
Abhinav Shashank
What makes anyone identify the best health plan for themselves? In today’s world, having health insurance is very important. You might end up paying significantly more for a doctor’s visit if you don’t have insurance than if you had it. You could rack up paying hundreds of dollars for a major injury or if you go for a costly treatment. And in this flock of health insurances, employer-sponsored health plans make up a significant percentage.
How does employer-sponsored health plans fit into the situation?
Employee health and well-being is not just essential, but also foundational to business success. Only a healthy team could deliver profitable outcomes. For this reason, among the list of many, most of employed Americans have their health insurance covered by their employers.
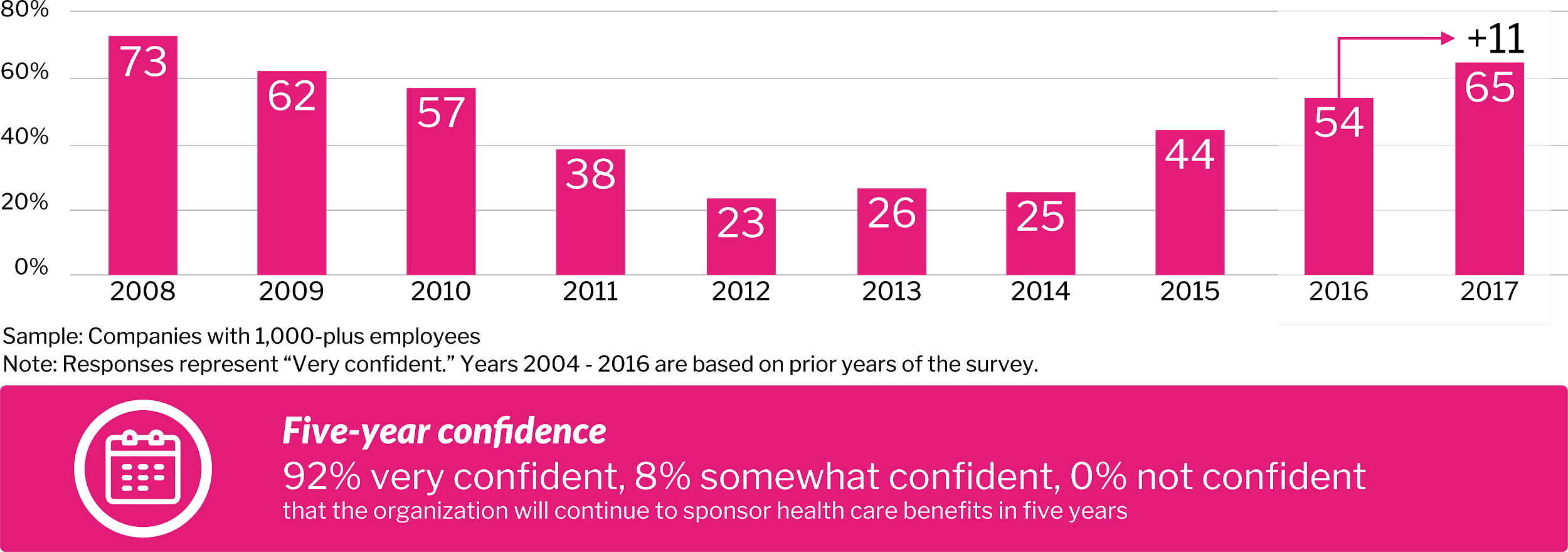
According to a survey, 92 percent of respondents were confident that their organization will continue to sponsor health care benefits for the next five years.
High-performance Insights- Best Practices in Health Care, 2017 22nd Annual Willis Towers Watson Best Practices in Health Care Employer Services
Is employer-sponsored healthcare on the verge of breaking or is it broken already?
Employer-provided healthcare is underleveraged. Currently, employer-sponsored healthcare is facing a lot of complications, including:
New market entrants add more complexity to employer decisions
As financial responsibility for care shifts to employees, an increase in self-rationing may drive poor outcomes
Pharmacy remains an area of unchecked rising cost, especially with regard to high- cost biogenetic (specialty) drugs, among many
What is haunting the large employers and how is the market ripe for innovation?
“Interestingly, 70 percent of employers believe new market entrants from outside the healthcare industry are needed to disrupt health care in a positive way. These disruptors include innovators from Silicon Valley and elsewhere, and employer coalitions,” said Brian Marcotte, president and CEO, National Group on Health.
Fifty-five percent of employers are concerned about prescription opioid abuse and working with partners to implement safe prescribing patterns and alternative therapies. The innovation we need to resolve this issue starts with data. With the launch of CURES 2.0 database, healthcare in the state of California achieved a milestone in curbing the opioid epidemic.
The role of activated data in enhancing the employer-sponsored health plan is that of an initiator to a revolutionary change in the field. Once the organizations have the right data, they can gain crucial insights into their employees and devise better plans to enhance their health and productivity.


 An effective advertising and marketing plan for the head and neck surgeon can capitalize your diverse capabilities. Head and neck surgeon needs successful marketing strategies while strengthening and building their practice. With advertising and marketing, you can get the advantage of a widespread opportunity spectrum. The head and neck surgeons deal with disorders of tongue, jaw, neck,
An effective advertising and marketing plan for the head and neck surgeon can capitalize your diverse capabilities. Head and neck surgeon needs successful marketing strategies while strengthening and building their practice. With advertising and marketing, you can get the advantage of a widespread opportunity spectrum. The head and neck surgeons deal with disorders of tongue, jaw, neck,