The days of life science companies focusing on physicians and medical professionals as their main “customers” are numbered. Larger healthcare market trends, better access to real world data and increasing costs are driving the shift to a new customer – the patient.
As total spending on medicines globally reaches the $1 trillion level annually, payers are, not surprisingly, placing greater emphasis on ensuring they are receiving value for their investments. Payers are bringing closer scrutiny to all parts of the healthcare system they are funding. Patients, too, are spending more in today’s system and in turn are changing their expectations about value and outcomes. As a result, we are seeing a new focus on real world evidence as payers and patients seek proof that the medicines are contributing to improved patient outcomes, reduction in hospital admissions or re-admissions, and more efficient use of resources.
In response, life science companies are seeking new and more effective ways to leverage data and analytics across the clinical-commercial continuum and to adapt their go-to-market strategies to reflect their focus on patient outcomes. Capturing results-oriented data and making it usable is critical for this new model to work and for the patient to receive the most appropriate care.
With this shift to outcomes-based results and real world evidence, many questions arise around the data and analytics. Who defines “value” and what does success look like? Is it long-term value or short-term results? Additionally, how should this information be distributed to and evaluated by the various stakeholders? How do we achieve a level of consistency when data sources are not yet fully interoperable?
As the pharma industry starts to work through the answers to these questions and begins to redefine go-to-market strategies and commercial models, effective utilization of data and analytics will prove to be one of the greatest competitive advantages.
Defining Value in the New Healthcare Era
This focus on patient outcomes has broader implications for the industry with data sources now being aligned with the patient to enable decisions across the enterprise including drug development, market access, and commercial performance.
Despite this ongoing trend towards employment, many physicians believe this is going to turn around. And if the industry is going to manage costs and improve outcomes, more private practices may be needed. According to an article in the New York Times, the cost of providing care in the hospital setting is considerably more expensive than the care provided in the smaller practice setting.
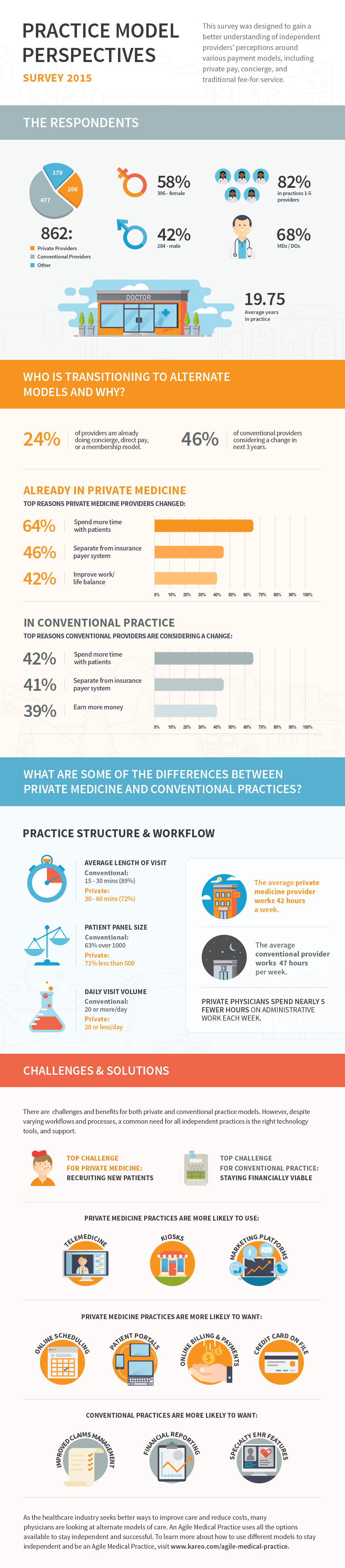
One of the ways physicians are finding to stay independent is through the use of private pay, or membership, models. Recently, the American Academy of Private Physicians and Kareo conducted the largest industry survey on physician perspectives on practice models. It showed that about 24 percent of providers have already fully changed or incorporated in some way a concierge, direct pay or membership model in their practice and another 46 percent are considering a similar change in the coming three years.
This infographic highlights some of the other key discoveries made in this industry-first survey.
Guest post by Chris Strammiello, Vice President of Global Alliances & Strategic Marketing, Nuance.
Chris Strammiello
The growing use of smart devices at the point of care exacerbates the dual, yet contradictory, challenges confronting hospital IT directors and compliance officers: Making patients’ health information easier to access and share, while at the same time keeping it more secure.
A major problem is that there are just too many touch points that can create risk when sharing protected health information (PHI) inside and outside of the hospital. In addition to securing communications on cell phones, tablets and laptops, these tools can send output to smart multi-function printers (MFPs) that not only print, but allow walk-up users to copy, scan, fax and email documents. This functionality is why the Office of the National Coordinator for Health Information Technology now defines MFPs as workstations where PHI must be protected. These protections need to include administrative, physical and technical safeguards that authenticate users, control access to workflows, encrypt data handled on the device and maintain an audit trail of all activity.
Accurate, Effective and Secure Use of Patient Information at Point of Care
Hospitals need to adopt an approach that automatically provides security and control at the smart MFP from which patient information is shared and distributed. This approach must also support the use of mobile computing technologies, which are helping to bring access to patient information and electronic health records (EHR) to the point of care. Advanced secure information technology and output management solutions can help hospitals protect patient health information as part of achieving HIPAA-compliant use of PHI with software by adding a layer of automated security and control to both electronic and paper-based processes. These solutions can minimize the manual work and decisions that invite human error, mitigate the risk of non-compliance and help hospitals avoid the fines, reputation damage and other costs of HIPAA violations and privacy breaches.
With this approach, vulnerabilities with capturing and sharing PHI are reduced with a process that ensures:
Authorization — only authorized staff can access specific devices, network applications and resources with password or smartcard based authentication. Network authentication is seamlessly integrated with the document workflow and to ensure optimal auditing and security, the documents containing PHI are captured and routed to various destinations such as email, folders, fax and EHR systems.
Authentication — user credentials must be verified at the device, by PIN/PIC code, proximity (ID), or by swiping a smart card access documents containing PHI. Once authenticated, the solution controls what users can and cannot do. It enables or restricts email or faxing and prohibits documents with PHI from being printed, faxed or emailed.
Encryption — communications between smart MFP’s and mobile terminals, the server and destinations, such as the EHR, are encrypted to ensure documents are only visible to those with proper authorization.
File destination control — simultaneously monitors and audits the patient information in documents, ensuring PHI is controlled before it is ever gets to its intended destination.
Content filtering — automatically enforces security policies to proactively prevent PHI from leaving the hospital by filtering outbound communications and intercepting documents – rendering misdirected or intercepted information unreadable to unauthorized users.
Guest post by Michele Hibbert-Iacobacci, CMCO,CCS-P, vice president of information management support, Mitchell International.
Michele Hibbert-Iacobacci
Recent ICD-10 end-to-end testing conducted by CMS and the American Medical Association yielded an 87 percent claim acceptance rate. This means that of the 29,286 test claims received, only 25,646 were accepted. Imagine thousands of claims denied due to providers submitting improper codes, stalling the bill review process and creating pain for everyone involved.
The one percentage drop in claims accepted from the month prior is a poor indication for the months ahead, as 100 percent of the test participants claimed to be fully ready for the October 1 ICD-10 implementation date. It’s only logical that many carriers and providers wonder what will happen to those that aren’t ready.
The end-to-end testing results also raise complicated questions: Which ICD-10 codes will be seen most frequently post-implementation date? And will these codes match what providers will put on the bills they send?
It’s no secret that ICD-9 has a lot fewer codes than ICD-10 and a situation is simply less complicated with less contextual data to worry about. As a result of the influx of new codes presented by ICD-10, we can expect to see providers assigning way more codes than necessary to bills in a pin the tail on the donkey-type attempt to choose the right code. For example, there are ten codes for a fracture to the tibia in ICD-10, as opposed to one in ICD-9. So many options may lead a provider to place all ten on a bill, to ensure payment is received.
It will be challenging for untrained providers to submit the correct ICD-10 codes, and as such, productivity will decrease alongside increasing reimbursement challenges and potential claim denials. Carriers, on the other side, will be forced to conduct extensive reviews of each bill to determine the actual injury cause and appropriate code.
To handle the huge influx of ICD-10 codes, providers can design a system where the office coders are provided with quick references to the most prevalent codes used in the practice. Over time, the overall billing experience will improve as coders become more skilled in identifying proper codes and carriers become more precise in reviewing bills. At first, carriers will be tolerant toward the reporting of multiple or vague codes. However, with each passing day post-implementation of ICD-10 carriers will become increasingly strict. Providers will be required to submit correct coding pending the value provided by the classification system accurately describes patient conditions.
This article is part of the “Think Further” series sponsored by Fred Alger Management. For more “Think Further” content, please visit www.thinkfurtheralger.com.
There is almost nothing I’m certain of except that life is an uncertain thing and that it seems to change a lot. Even in the most predictable of settings, even the minutest changes in detail can have a lasting and overwhelming effect on nearly everything in its atmosphere. In healthcare, a space seemingly immune to the status quo, things seem to get a whole lot more complicated. The same can be said of life and death, health and well-being. On their own, they are not so difficult to understand and often, in most cases, predictable and redundant; until the final days, of course, then things begin to get a little more complicated. When we’re fine, we’re fine. Life is good and most of our concerns seem trivial.
Then health gets involved and the minutest change in detail can send our lives in a spiral so much so that we barely recognize our place in it let alone who we are and where we belong. When such an occurrence arises, we begin to rely on beeps and buttons, software and technology in ways never before imagined for the intersection of our lives.
Clearly, the health IT landscape will be completely different five years from now. From where we stand today to where we’re headed, we’ll likely look back on this moment and wonder how we survived such archaic times. Just a couple years removed from the age of the electronic health records, technology that already seems dated and antiquated, is no longer monolithic and domineering to the space as it likely seemed in 2010.
Our future selves might stand on the threshold of 2020 and say that we were being single minded. The technology — EHRs were supposed to save healthcare and are now nothing but foundational. The technology was supposed to simply aggregate information collection, provide for the ability to quickly share information system wide and around the world; and give us the capability accessing all of a patient’s information at the tips of the proverbial finger.
When the promise of those solutions faded (yes, their stars have faded) and as our attention forced us into new technologies (primarily because of consumers’ desire) we are now seeing developments in technology creating touch points that impact patients “where they live” and has become the new force behind healthcare technology.
Consumers will drive healthcare’s future. Probably not a secret at this point, but a point that is hard for the old guard. They’ve had enough of being left out of the ownership process regarding their own health. They’re tired of being locked out of their own records, and kept access to their own information. Such data would not exist without those helping produce it. New consumer technologies have and will further level the field. Consumer tech will continue to spur innovation, at light speeds. Data will flow between healthcare parties and its consumers; HIPAA protections will be waived and open access for the social good will become the norm. Standard and traditional approaches when dealing with patients, in a generation or so, will be completely different and far less segmented, as they are now.
Guest post by Renata Magurdumov, director of marketing, ColoGuard.
Renata Magurdumov
If you think about it, your doctor probably knows more about you than many of your friends. Healthcare providers store a ton of sensitive data about their patients; everything from their name to their address and place of employment to their Social Security number. In other words, everything a cyber-criminal would need to steal someone’s identity.
Given how valuable that information could be in the wrong hands, you’d think that healthcare providers would use the most high-tech, modernized infrastructure and the most up-to-date security practices to keep it safe. Unfortunately, you’d be mostly mistaken.
Recently, Premera Blue Cross was the victim of a ‘sophisticated cyberattack’ that compromised the healthcare records of 11 million patients. Before that, the victim was Anthem. Before that, Aventura Hospital and Medical Center.
As a matter of fact, according to a recent Kroll study, healthcare accounted for nearly half of the client breaches that took place in 2014, followed closely by business services and higher education. This was the second year in a row that these three industries accounted for nearly two-thirds of all “client events.” What’s more, only 30 percent of the breaches in healthcare were the direct result of hacking.
That means that the other 70 percent were the result of human error – of negligence, poor security practices or ignorance. For an organization whose collection of data can quite literally ruin lives by falling into the wrong hands, this is unacceptable. And it’s going to get worse before it gets better.
“I believe that healthcare IT systems are fragile and highly vulnerable today,”writes CIO Paddy Padmanabhan. “This, combined with the sophistication of hackers and the rising attractiveness of healthcare data in the black market, makes healthcare a huge target for disruption in 2015.”
The Rocky Relationship Between Healthcare and IT
Part of the problem is that many decision makers in healthcare have a serious attitude problem where technology is concerned. They simply don’t realize how important it is. Healthcare IT is often marginalized and undersold, with CIOs struggling simply to keep their departments afloat – if it’s not simply contracted out to third parties.
“While healthcare costs in the US as a percentage of GDP are the highest in the world, healthcare IT spend as a percentage of revenues is among the lowest across various industry sectors,” continues Padmanabhan. “Healthcare CIOs are constantly challenged to do more with less, and face budget cuts year after year.”
The end result of this is that many hospitals view technology as a hindrance. It’s obtuse, frustrating and poorly implemented – because their IT departments lack the resources to make it anything but. Writing for the New York Times, leading healthcare analyst Robert M. Wachter recounts how a job ad last year listed the fact that it didn’t have digital databases as a plus.
“In today’s digital era,” writes Wachter, “a modern hospital deemed the absence of an electronic medical record system to be a premier selling point. That hospital is not alone.”
“A 2013 RAND survey of physicians found mixed reactions to electronic health record systems, including widespread dissatisfaction,” he continues. “Many respondents cited poor usability, time-consuming data entry, needless alerts and poor workflows.”
Worse still, even those hospitals that have successfully implemented modern IT are fighting an uphill battle to figure out how it all works. They grew so accustomed to the way things were, says Wachter, that they found themselves utterly unprepared for a shift which was, for all intents and purposes, years in the making. They were complacent – and now they’re paying for it.
“Whopping errors and maddening changes in workflow have even led some physicians to argue that we should exhume our three-ring binders and return to a world of pen and paper,” he says. “That argument is utterly unpersuasive. Healthcare, our most information-intensive industry, is plagued by demonstrably spotty quality, millions of errors and backbreaking costs. We will never make fundamental improvements in our system without the thoughtful use of technology.”
In 2013, while searching for a telemedicine solution, Brandon Welch thought that his only options were expensive and complicated telemedicine systems or video conferencing solutions that were not HIPAA compliant. He wondered where he would find simple and free telemedicine solutions. He said he felt, “The world needed a simple and secure telemedicine solution that was freely available to all healthcare providers.”
So he created Doxy.me.
Elevator pitch
Telemedicine will revolutionize the delivery of healthcare by making it more convenient and accessible for patients to access qualified healthcare professionals, and reducing unnecessary expenses. Unfortunately, current telemedicine technologies are expensive and complicated to use, limiting its widespread impact on healthcare.
For telemedicine to change the world, we believe that telemedicine technologies must be simple and free to use. That’s why we developed Doxy.me — the simple, free, and secure telemedicine solution.
Product/Service Description
Doxy.me is a simple, secure, HIPAA-compliant and free telemedicine available to an clinician in the world. They can use the platform to provide care to their patients, or use it for clinical research or clinical trials.
Origin Story/Founder’s Story
Brandon Welch
Doxy.me was founded at the University of Utah by then Biomedical Informatics PhD student Brandon Welch while working on a research project within Department of Obstetrics and Gynecology. The goal of the study was to develop and evaluate a novel prenatal care delivery model that replaced several in-person prenatal care visits with telemedicine visits with pregnant moms from home or work. Initially, he wanted to use Skype or FaceTime for the technology, but the institution wouldn’t allow it because these popular and free conferencing solutions were not deemed to be HIPAA-compliant. So he set out to find a good, simple and free telemedicine solution. However, he was surprised upon reviewing HIPAA-compliant telemedicine technologies that the only options available were complicated and expensive; none were deemed practical to be used by patients at home. Being familiar with the technology, he set out to build a simple and free telemedicine solution. He first submitted the idea to a medical invention competition at the university and won the “Consumer’s Choice” award, and he used the winnings from the competition to build the first prototype of Doxy.me (which was used in the prenatal care study). Over the next year, he continued to improve the Doxy.me features based on clinician and patient feedback, but with a guiding principle of simplicity and ease of use.
Marketing/Promotion Strategy
Since it was officially released to the public, it has grown exceptionally over the past year with little marketing efforts. Networking with organizations and word of mouth has been the largest marketing tool.
Market Opportunity
Competitors include snap.md, telehealth.org and vsee.com. Market opportunity really focused on the fact there were no telemedicine solutions that were HIPAA-compliant, free and easy to use. This gave us a leg up on our competitors, as most other solutions require downloads, plug-ins, or are expensive.
Every time a person seeks medical treatment, healthcare professionals are required to use a specific code for billing and tracking purposes. The International Classification of Diseases, Revision 10 (ICD-10), was launched Oct. 1, 2015 — after 20 years of delays.
The new ICD-10 codes multiply the medical coding options available by a factor of five, jumping from roughly 13,000 diagnostics codes under the ICD-9 to more than 69,000 with ICD-10.
ICD-10 attempts to label every possible diagnostic scenario imaginable. Whether you’ve had an initial encounter with an orca whale (W56.21XA, W56.22XA or W56.29XA) or an unlikely repeat orca encounter (W56.21XD, W56.22XD or W56.29XD), been injured by a brass musical instrument (Y93.J4), or walked into a wall (W22.01XA, W22.01XD or W22.01XS), believe it or not ICD-10 has a classification for it.
Don’t believe us? Take a peak for yourself. Check out the ICD-10 Code Lookup Database or you can just look at the entertaining graphic below provided by Quill.com. The graphic illustrates 14 funny examples of ways people injure themselves and how ICD-10 classifies them.
A personal favorite? It has to be V91.07XA: Burn because of to water skis on fire, initial encounter. It’s easy to wonder how this happens once, let alone more than once, V91.07XD: Burn because of water skis on fire, subsequent encounter.
Take a look at the following graphic depicting some of the most bizarre ICD-10 codes, thanks to and provided by Quill.com. What will these codes, when aggregated over the next few years, say about us as a people? That we’re likely into, and injured by, some pretty weird stuff! Perhaps I’ll write a book.