About two decades ago who would’ve thought of the invention of Nano robots that are able to carry drugs all the way to the human bloodstream?
It’s happening. Technology is revolutionizing the conventional ‘human country doctor’ health care and there’s not much to be surprised of. With modern machines and software taking over the healthcare industry, one often wonders, “What good is technology doing to it?”
Health information technology (HIT is information technology applied to health and health care. It supports health information management across computerized systems and the secure exchange of health information between consumers, providers, payers, and quality monitors) is the burgeoning specialized combination of information technology, communications, and health care and it is altering the course of patient care for the better. Here’s how:
Knowledge Sharing
Practicing medicine is a lifelong learning. Doctors need to be on their toes all the time to acquire the knowledge of the latest developments in their field. Not updating themselves can make their practice stagnant – nobody would want to consult a doctor like that. Health IT brings the knowledge about everything, be it patients, therapies, diseases or medicines at their easy disposal. This knowledge can be easily shared between consultants, patients, and can even be updated when needed. That’s a whole new world of medical science for the doctors and patients to explore.
Improved Coordination
The world is swiftly moving towards specialization. Healthcare is no different. A single hospital stay could mean being under the observation of several different specialists at the same time. These specialists are required to coordinate with each other on every case they deal with. The way forward is paved by health IT. Health IT helps bring everything related to your condition from nutrition to neural complications in tandem with each other. The specialists know which condition can make regular course of treatment difficult for you or which medicine would trigger your skin allergies. The result? There are fewer chances of problems arising in your healthcare.
Better Outcomes
The most significant way IT is transforming the healthcare industry is in the form of better outcomes. Automation streamlines the operations of a medical facility, making them more effective and efficient. It is easier for different doctors and nurses to coordinate and diagnose a particular case. There are less chances of human error which ultimately leads to higher quality and safer care. With less time wasted in going through physical files and other manual work, doctors and nurses have more time on their hands to spend with patients.
The Patient’s Involvement
If anything, health IT has made patients increasingly vigilant about their health. It enables them to gain electronic access to their medical history, health records, and doctor’s recommendations. They get a chance to take control of their health. Patients’ portals and online knowledge hubs help patients educate themselves about their conditions, its symptoms and treatment procedures. Health IT makes it easier for patients to get in touch with doctors and nurses for better health outcomes and medical care.
In the age of the digital hospital and the connected patient, security will likely improve the less it depends on providers.
Everything from HIPAA to patient engagement treats physicians as the white hot sun of the healthcare universe, holding everything together and keeping it all in stable orbit. They are accountable for health outcomes, for patient satisfaction, for guiding patients to online portals, and for coordinating with care teams to keep data secure — even as mobility and EHR dominance complicates every node in the connectivity chain. All this digital chaos brings more diminished security.
Only as Strong as the Weakest Link
Every business out there has learned — usually the hard way, or by watching someone else learn the hard way — that whatever the security infrastructure, users are the weakest link. More devices means more users, and more connectivity and data-sharing means more weak spots all along the chain. By design, the EHR system adds vulnerability to healthcare data security through a long chain of users.
Patients don’t have a systemic, accountable role in all of this. Our whole approach fosters passivity on the part of the patient and paternalistic assumptions on the parts of caregivers and policymakers. We give tacit acknowledgement of this imbalance whenever malpractice law or tort reform is mentioned — and promptly left behind in the face of other, patient-exculpatory programs and initiatives.
Patients are a part of this. Clearly they are invested in their own security — the costs of health data breaches contribute to the rising costs of care, besides exposing personal financial and medical information that can carry its own universe of costs.
Patients are implicated, but they must also be accountable for security in the new high tech healthcare system.
An Old Problem with New Importance
Getting patients included in the evolution and delivery of healthcare requires engagement. The same goes for digital security. The ethical and financial dilemmas of the security situation is an expensive distraction for administrators and caregivers, but it is a learning opportunity that could empower patients. A new emphasis on digital security and privacy could be the start of a cascade of engagement with further questions of use and responsibility for outcomes.
Already, patients are key players in making telemedicine effective. Access is on the shoulders of the patients, and utilization depends on their technical literacy. The incentives–time and money savings, improved access to care–are powerful, but come with the obligation to learn the platform through which remote care is delivered. Utilizing any telehealth solutions requires patients to think about what information they want to share, whether they trust the new platform, communicating effectively with their provider, and gaining confidence for the new medium.
This same model can be applied more broadly to EHRs, and the patient role in the digital healthcare system.
Guest post by Lea Chatham, editor-in-chief, Getting Paid, a Kareo Resource.
Lea Chatham
Patient engagement has been the hot topic of this past year or two. Everyone agrees that engaging patients more in their healthcare can help reduce costs and improve overall health. A study conducted by HIMSS in 2015 showed that the majority of physicians believe patient engagement is beneficial and should be a part of their job. However, the study also concluded that over 40 percent of physicians worry that there is little reimbursement for engagement activities.
Patient are looking for more ways to connect with providers from online scheduling to text reminder to email follow ups and social media. And while many see these as conveniences, the reality is that they do also improve health and have the potential to reduce costs. Studies have shown that simple follow up communications via text and email can help ensure patients show up for appointments and can reduce hospital re-admissions, which has a big impact on healthcare costs.
Unfortunately, physicians are already stretched thin trying to care for patients, run their practices, adhere to complex programs like meaningful use and PQRS, and navigate changes like ICD-10. Who has the time to do more? And many providers worry that “engagement” means more work with less reimbursement. But it doesn’t have to be that way.
In fact there are many opportunities to automate engagement and provide the tools patients want without adding any time or effort to a provider’s plate. Today, there are solutions that once set up enable easy online scheduling, text and email reminders, follow up patient surveys, and even re-care programs.
This infographic highlights some of the feelings of both patients and providers feel about patient engagement and shows how practices can utilize engagement strategies that benefits both and do have a financial return.
Guest post by Mark Ott, vice president of product, RoundingWell.
Mark Ott
As 2016 unfolds, the move from fee-for-service to value-based care is entering a more advanced stage. As the process evolves, priorities for healthcare providers of resources, teams and tools becomes more convoluted. To keep on track, both for healthcare organizations and CMS changes, providers should keep in mind the following:
The care management/coordination record rises in importance, especially as team-based care models expand
Some call it a care management medical record and others call it a care coordination record. Regardless of the term, the concept is essentially the same. EHRs are basically encounter management systems, but as care expands beyond the in-person encounter, capturing and tracking what happens between patient visits will be of utmost importance. In addition, enabling care teams to stay on the same page about a patient’s care plan, track action steps, and reduce the friction of working together will be crucial to succeeding in a value-based world. Expect to see the Care Management Record concept start catching fire in 2016.
Demand will increase for consumer-grade user experiences in healthcare enterprise software
For so long, clinicians on the frontlines of care delivery have had to struggle with software that’s hard to use, difficult and downright frustrating. The biggest culprit for poor user experiences in healthcare software has to do with the enterprise purchasing process. Vendors build for buyers, like the C-suite, who aren’t also the end users. If the end user and the buyer were the same, you’d see healthcare software vendors value user experience like what we see in other B2B industries, not to mention B2C industries. Regardless, in 2016 we will see more buyers value products with consumer-grade user experiences. Much of this has to do with end users’ reluctance and sometimes outright resistance to adopting technology in their worklife. Clinicians often get a bad wrap for being technology averse. But in reality, it’s not that they’re averse to technology; it’s that they’re averse to bad technology.
Integrating wearables and their data into care delivery processes will remain a niche activity
The enthusiasm around wearables, trackers and remote monitoring is exciting and there is enormous potential for device data to impact the delivery of care in ways that benefit both patient and provider. But the technology hasn’t caught up with the promise of what they can be, and that won’t change in 2016. Not only is the technology not yet able to deliver, but the incentives and processes to support wide-scale deployment are not in place yet. Though all signs point to wearables becoming an integral part of delivery of care, this won’t happen next year.
Telemedicine technologies are evolving rapidly, enabling better care, greater patient access and the promise of bending the healthcare cost curve. Telemedicine has evolved dramatically over the past few years, and providers have come to realize the profound ways in which it can improve patient care. With this evolution has also come the increasing sophistication of telemedicine practitioners. Doctors, nurses and administrators now desire easier integration, clinical adaptability and configurability, support for multiple specialties on a single comprehensive platform, and robust data collection and analytics.
REACH Health, a leading provider of enterprise telemedicine solutions, has identified five key technology trends for the coming year, each promising benefits for providers and patients. These trends for 2016 include:
Obsolescence of Proprietary Hardware and Networks: Although proprietary hardware and networks were standard in the early generations of telemedicine technology, healthcare providers now desire affordable, flexible solutions. Effective telemedicine programs are increasingly powered by off-the-shelf PC components, standard, low-cost cameras and emerging networking standards such as WebRTC. These open, standardized products allow providers to choose the most appropriate end-point for the clinical need; whether it be a high performance cart, a PC or a mobile device such as an iPad, Android or Surface tablet. Providers also now increasingly seek specialty-specific telemedicine software applications that are deployable across these commodity hardware devices using open networks.
The Rise of the Software Platform: Healthcare systems now seek enterprise-wide telemedicine solutions that can be scaled to support multiple service lines and a variety of delivery models, all on one common platform. Just as single-function “dumb phones” have been rendered obsolete by multi-purpose “smart phones,” providers want a single platform to accommodate all their telemedicine needs. They expect a simple, effective solution that supports varied telemedicine requirements across the continuum of care and works wherever it is needed, on a variety of devices. These platforms must also be designed with an open architecture, providing the ease of plug-and-play connectivity with specialized, interoperable components such as high quality peripherals.
As the excitement of the festivities continued to roil on in Chicago for the annual Healthcare Information and Management Systems Society (HIMSS) conference, and as health systems leaders merged with colleagues and partners for what is health IT’s biggest event of the year, I was not among those in attendance. As the conference opened and buzz at the show began to swell, excitement for news and new developments flowed from nearly every available channel, I was back home, far from the excitement of the show or its announcements, developments and news makers.
As health system leaders and their technology partners discussed how their solutions could make care better, engage patients more effectively and lead to better outcomes, greater efficiencies and higher quality care, my wife and I were in the center of the care universe in the heart of our local hospital where I was helping her through the delivery of our second child. Though the process was relatively straight forward and was done very quickly, the experience made me realize several things about healthcare technology from the patient’s perspective.
The first thing is that no matter how important we claim the technology used in the care setting to be, it matters little to those receiving care. For those receiving care, they want and need a seamless process where they have immediate access, without a wall of technology between them, to their care providers whether that’s a nurse, physician or some other support personnel. Patients, at the point of care, don’t want to face the burdens of interacting with the technology their caregivers are concerned with, but we as patients want their full attention. If patients must break through a fourth wall of technology, as I’ve seen to be the case on more than one occasion, the care staff, and more importantly, the health system, has failed the patient.
Secondly, patient engagement is more than a portal or access to one. And while patient engagement means different things to different provider types – like ambulatory vs. in-patient –the patient is still at the heart of the care, not the technology. Those who believe that technology can solve the patient engagement ills are wrong, and likely are failing to truly engage patients because they believe the myth that it can. Perhaps meaningful use has bastardized the term “patient engagement,” but it’s a sad thing when the entirety of that conversation centers around some form of technology or device. The irony of an event like HIMSS, where most of health’s relevant vendors clamor to meet with health system leaders, is that the buzz is built to surround the movement of the patient. The patient is at the heart of care, not technology or some bolt-on software solution.
We, patients, have been at the heart of care since the existence of healthcare; technology is an infant at play here. Let’s not forget that.
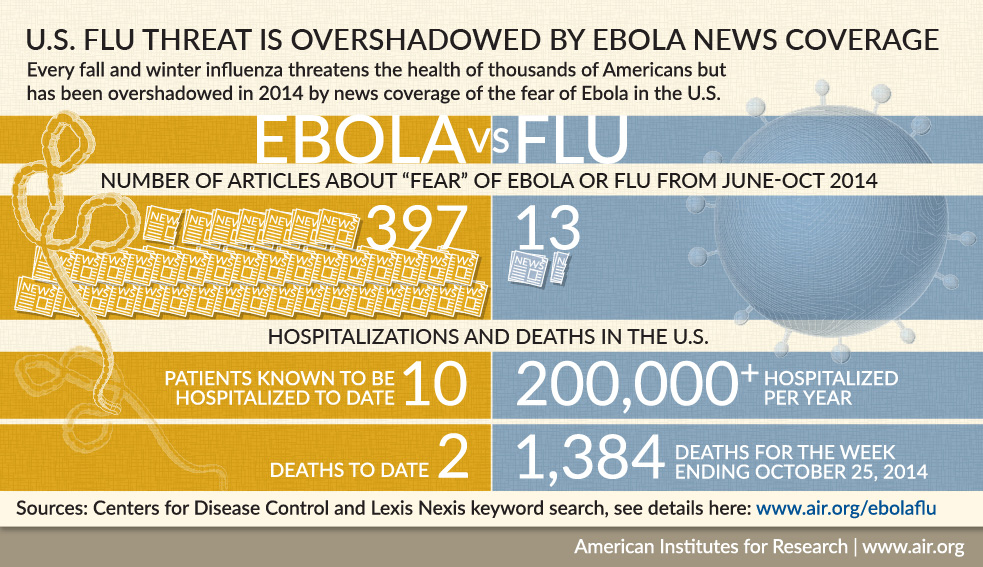
Two big communicable disease scares—Ebola and measles—gripped the attention of the general public recently. They did so with enough strength that the average person on the street spoke out and demanded that actions be taken to protect themselves and families. It was virulent on social media. The total count of Ebola deaths at the end of last year was 5,021 worldwide. The CDC reported 10 Ebola cases treated in the U.S. and two patients died as of January 2015. There were 121 total measles cases in the U.S. this year in 17 states. All but 18 of the measles cases were because of an outbreak that spread from Disneyland in California.
What is remarkable is that these two infectious diseases affected a total of less than 200 people across the nation. Yet it triggered a vigorous response from masses of people who were afraid that they could contract Ebola when the actual chances were significantly lower than dying from a lightening strike. The spread of measles among children erupted into online wars between the vaccinated and unvaccinated.
Contrast this with the lack of concern over the flu vaccine’s low effectiveness against this year’s virus, which the CDC estimates kill 3,300 to 49,000 people in the U.S. every year. Warnings from the CDC that the flu strain this year is worse and getting the flu shot will at least temper the illness seems to have had little effect on increasing vaccinations.
Ebola attracted the public’s attention with such obsessive coverage that the public expected exposed individuals to be quarantined even though an individual had no symptoms to indicate a contagious state. More importantly, contact with fluids of an infected person is necessary to become infected. Contrast this with measles where the air and surfaces an infected person has coughed or sneezed remain contaminated for up to two hours. Measles is contagious up to four days before the telltale rash appears. According to the CDC, about one in every 1,000 children who contract measles will die and 90 percent of the non-immune people close to an infected person will get it.
Fear was the driver for Ebola’s patient engagement. The measles outbreak engaged parents because it raised the issue of the high rate of non-immunized children of a highly contagious and serious disease, but there were no calls to quarantine measles victims and guard them as with Ebola victims.
According to Patient-Centered Primary Care Collaborative, the patient-centered medical home (PCMH) is a “model or philosophy of primary care that is patient-centered, comprehensive, team-based, coordinated, accessible, and focused on quality and safety.” PCMHs power business and clinical processes by using clinical decision support tools to connect patients with members of their healthcare team to improve both the patients’ and the providers’ experience of care. This coordination encourages a stronger physician-patient relationship, leading to better care delivery, more involved and engaged patients and reduced avoidable costs. According to the National Committee for Quality Assurance (NCQA), these models are “transforming primary care practices into what patients want, focusing on patients themselves and all of their healthcare needs. They also are foundations for a healthcare system that gives more value by achieving the ‘triple aim’ of better quality, experience and cost.”
The NCQA recognizes over 10 percent of U.S. primary care practices as patient-centered medical homes. In order to be recognized by the NCQA, these primary care practices must offer access both afterhours and online, allowing patients to receive care when and where they need it. They work with patients to make treatment decisions based on individual preferences and help patients engage in their own health. The practice as a whole works as a team to coordinate care from other providers and community resources to maximize efficiency. Additionally, PCMHs focus on preventive care and the management of chronic conditions to prevent complications and emergencies.