Guest post by James Hofert, Roy Bossen, Linnea Schramm and Michael Dowell of Hinshaw & Culbertson.
In 2013, healthcare industry stakeholders, including associations, EHR vendors, practitioners and providers, raised significant concerns relating to the implementation timing of meaningful use Stage 2 and 3 criteria, including problems with interoperability, usability and regulatory failure to assess “value added” by implementation of meaningful use criteria to date. On December 6, 2013, federal officials announced that Centers for Medicare and Medicaid Services (“CMS”) were proposing a new timeline for the implementation of meaningful use stage criteria for the Medicare and Medicaid Electronic Health Record (“EHR”) incentive programs. The Office of the National Coordinator for Health Information Technology (“ONC”) further proposed a more regular approach for the update of ONC’s certification regulations.
Under the revised timeline, Stage 2 will be extended through 2016 and Stage 3 will begin in 2017 for those providers had completed at least two years in Stage 2. The goal of the proposed changes is twofold; to allow CMS and ONC to focus efforts on the successful implementation of the enhanced patient engagement, interoperability and health information exchange requirements in Stage 2, as well as evaluate data from Stage 1 and Stage 2 compliance, to date, to create and form policy decisions for Stage 3.
Roy Bossen
CMS expects to release proposed rulemaking for Stage 3 in the fall of 2014, which may further define this proposed new timeline. Stage 3 final rules would follow in the first half of 2015.
Despite CMS’s positive response to stakeholders concerns relating to the timeline for implementation of Stage 2 and Stage 3 meaningful use criteria, significant reservations continue to be enunciated, on a monthly basis, by providers at both Health information technology (“HIT”) policy committee and work group meetings. Providers continue to urge rule makers to institute consensus standards that could be adopted broadly across the healthcare industry to ensure both usability and interoperability.
In early 2013, former national coordinate Farzad Mostashar chastised electronic health record vendors for improper behavior in the marketing and sales of systems that continued to frustrate interoperability goals. This frustration with EHR vendors continues to be enunciated in HIT policy committee and work group meetings as recently as January of 2014.
Dr. David Lischner started Valant Medical Solutions in 2005, a web-based EHR and practice management solution designed specifically for the mental healthcare practitioner. Because he went to school to practice medicine and not administer paperwork, he set about creating a tool that would not only afford him more time free from his practice, but also provide a secure record keeping solution that is integrated with a clinical support tool – allowing him to be a better doctor to his patients. Simply put, he and the team have developed a SaaS tool that intuitively enforces measurement based care.
Despite expert literature highlighting the potential importance of evidence-based-care in psychiatric practice, most doctors simply do not employ these measures. As we know, those physicians who don’t start showing off their patient outcomes to insurers are going to be weeded out by both the federal EHR incentive program and the Affordable Care Act. Valant provides this market, along with the early adopter forward thinkers with both useable solutions to age old problems and readied answers to future concerns — of which there are many within this industry, and this specialty particularly.
The following are his thoughts about EHRs, building a software business and why he chose to start Valant Medical Solutions.
As a practicing psychiatrist with a successful group practice, why did you venture into the EHR space and develop your own software?
I loved seeing patients. I loved being in private practice. But I wanted to have an impact on a larger scale. And, I also discovered that I loved starting and growing businesses.
I didn’t like the solutions that were out there to help me manage my practice. They were either focused on primary care and other specialties or too narrowly on just one type of mental health care provider or practice. I also saw that web-based software was beginning to transform business processes in other industries and thought that this must be possible in healthcare, and specifically in behavioral health care. Finally, and this was a more distant motivation, I wanted tools that made it easier or even fun to practice in an evidence based fashion.
An enterprise-wide data warehouse and a cross-functional team approach to analyze care delivery and protocols has enabled Texas Children’s Hospital in Houston to improve care and achieve millions of dollars in savings at the same time.
Implementing electronic health records was only a starting point for the process, says Myra Davis, senior vice president and CIO for the Houston-based facility. Analyzing the data from the EHR system and other information systems in the hospital with diverse team members using visualization applications has enabled significant improvements in clinical processes, she said.
The use of the data warehouse and improved analytical processes has strong support from clinicians and research specialists, who lauded the approach’s ability to conduct research.
“It’s great to be in a meeting to slice and dice the data,” said Terri Brown, research specialist and assistant director of data support at Texas Children’s Hospital. “When it used to take three months to get a report, now within 30 minutes you have such a great understanding of the data. It takes away the false leads. It tells you what the source of truth is for how we have changed care delivery. It has been revolutionary.”
Guest post by Tina Greene, senior regulatory affairs consultant, Mitchell International.
There are major healthcare regulatory mandates going in effect, at the federal and the state level, which will significantly impact property and casualty (P&C) insurance medical bills payers. The Administrative Simplification provisions of the Federal Health Insurance Portability and Accountability Act of 1996 (HIPAA, Title II), state mandates for property and casualty eBilling and more regulatory initiatives are forcing payers to understand these regulation’s requirements and be prepared to implement new processes and technologies in order to be compliant. Federal healthcare administrative simplification offers payers an opportunity to prepare for compliance while meeting cost containment and operational efficiency objectives, empowering property and casualty payers to prepare for an all-electronic American healthcare future.
The concepts of eBilling and ePayment for medical bills are gaining traction throughout the healthcare arena, along with the adjacent P&C insurance industry. Medical providers and P&C payers are increasingly taking advantage of the benefits associated with electronic billing and payments, which include substantially lower transaction costs, increased efficiency for call centers, adjusters and finance departments.
Non-legislative organizations are collaborating and recommending changes that could accelerate the impact on the P&C industry.
Other non-legislative organizations are collaborating and recommending changes that could accelerate the impact on the P&C industry. For instance, the Workgroup for Electronic Data Interchange (WEDI), the International Association of Industrial Accident Boards and Commissions (IAIABC), the American Medical Association (AMA), and the Accredited Standards Committee of the American National Standards Institute (ASCX12) are all working to ensure standards to facilitate eBill exchange and adoption. The National Committee on Vital and Health Statistics (NCVHS), a public advisory body to the Secretary of Health and Human Services (HHS), periodically holds meetings to review health statistics and trends. And while the NCVHS does not set policy, they do provide analysis, insight and recommendations to HHS, with eBilling as a topic of likely review in the future. These organizations have collectively laid a path for how to participate in this new environment.
Guest post by George Bailey, senior advisor, health IT/security, Purdue Healthcare Advisors.
The recent large-scale data security breaches experienced by major retailers Target Corp. and Neiman Marcus provide opportunities for learning across industries. These data breaches are painful for the companies, shareholders and, certainly, for the consumers victimized by subsequent fraudulent transactions on their financial accounts.
But once the dust settles, will these 110 million consumers suffer long-term damage to their privacy and financial security? I would argue no. Surprised? I say this because most of the attributes compromised in the Target and Neiman Marcus data breaches are short-lived items. By “short-lived,” I mean bits of information that can be changed or replaced by the consumer.
For instance, charge card numbers can be changed and accounts closed; debit card PINs can (and should) be changed; lost funds can be reimbursed; and credit scores reinstated. Now I don’t want to imply that this cleanup is easy, quick or inexpensive to do. It’s not. But looking three to five years into the future, these data breaches—just as the T.J. Maxx breach in 2007—will have little-to-no lasting effect on those compromised.
For the healthcare industry, a data breach is a quite different. A patient’s social security number (contained many times within healthcare records), medical history, psychiatric notes and sexual preference are not considered attributes that are “short-lived.” While a social security number can be changed, it’s a difficult and time-consuming process. The other data contained in a healthcare record is very sensitive, private, and cannot be re-written, as it is there to guide physicians in providing optimum care. Once sensitive electronic patient health information (ePHI) is lost, stolen or leaked to the Internet, it can spread faster than the best Facebook gossip and be cached, indexed and copied to a seemingly endless number of devices.
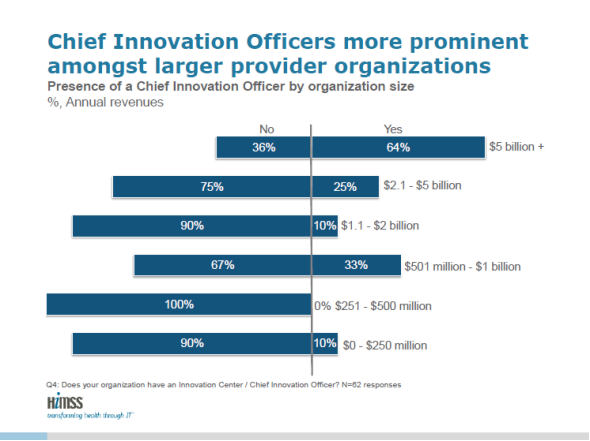
According to HIMSS, going beyond implementation of the electronic health record, healthcare providers increasingly look to innovation to reduce costs, improve patient care and increase patient safety. To learn more about how hospitals and health systems plan for, resource, and execute on their innovation agendas, HIMSS and AVIA launched the 2013 Healthcare Provider Innovation Survey. (Infographic below)
HIMSS and AVIA collaborated to produce the 2013 Healthcare Provider Innovation Survey, which was conducted by email from Aug. 20 to Sept. 30, 2013, with select U.S. hospitals, academic medical centers, children’s and ambulatory care centers to understand the current state of innovation within provider organizations. By analyzing the data collected from the 92 participants, HIMSS and AVIA determined the top barriers to innovation. The data is not necessarily meant to be representative of the market, but rather, facilitate dialogue about what the market is doing to determine the top barriers to innovation and other findings as reported in the results.
Eric Langshur, AVIA CEO, said: “The future of healthcare will be greatly influenced by providers’ ability to harness the latest technologies to positively impact their patients – and their bottom line.”
As most healthcare professionals know, an important step in the improvement of healthcare quality and cost will take place in October 2014, just under a year from now. This important step is the transition from ICD-9 to ICD-10 – with this new code set, the largest financial system change will take place since the Prospective Payment System (PPS) in 1983.
This change has to take place for several reasons including that with a maximum of 13,000 codes, ICD-9 is not specific enough for detailed diagnoses and the current codes do not reflect new services and technology in CMS payment systems. With more than 171,000 codes, ICD-10 will provide much more detailed clinical pictures and data, improving accuracy in all aspects of patient care. New data available through ICD-10 will help determine public health needs and identify trends, as well as helping to spot bioterrorism and epidemics.
The transition will not only impact healthcare organizations, but also physicians, for whom it will be particularly beneficial. Physicians will be able to determine the severity of illnesses more clearly, and, therefore, quantify the level of care more accurately. The codes will also create an electronic trail of documentation, which can help physicians receive proper payment and ensure their reputation remains in good standing.
With the importance and significance of this transition, it is crucial that ample preparations are made. However, there are many organizations that have not yet embarked on the road to preparedness and many concerns exist throughout the industry. For example, according to a survey conducted by the MGMA-ACPME of 1,200 office-based practices surveyed, approximately 70 percent of respondents were very concerned about expected loss of clinician productivity and the same percentage was very concerned about changes to clinical documentation. 71 percent surveyed responded that, in order to accommodate ICD-10, their EHR systems either were upgraded or still need to be upgraded, will need to be replaced, or they are unsure which. Only 0.6 percent had tested their EHRs for ICD-10 compliance.
Providence Hospital, located in downtown Columbia, South Carolina, is a 247-bed hospital founded in 1938 by the Sisters of Charity of Saint Augustine to minister to the community, in both body and spirit. The facility is best known for the expertise in cardiac care it provides through Providence Heart and Vascular Institute. With a hospital staff of more than 2,000 nurses, doctors and hospital administrators, Providence Hospital needed to standardize setup of user accounts and reduce the amount of time network engineers spent assigning rights in Active Directory.
Tony McNeil, technical manager said, “We have more demands on our department and we are not getting any additional staff because of the economic situation. Therefore, we have to work smarter and we need tools that help us work more efficiently.”
This became a perfect opportunity to put into action a permanent process for user account life cycle management utilizing Tools4ever’s complete User Management Resource Administrator solution.
Immediate delivery
Providence Hospital decided to implement UMRA to mainstream the provisioning process from the time an employee is hired and entered into the hospital developed, web based security application to the time they are entered into Active Directory. The previous process took nearly 2 days to complete before a user was ultimately provisioned in all systems. Now the process allows for an almost immediate creation of a user account with the correct provisioning. A web form allows for the assignment of group privileges and permissions to individual users. The application also creates the appropriate Exchange mailbox and creates a home folder for the employee on the appropriate share drive.