With the yearly bluster and promise of HIMSS, I still find there have been few strides in solving interoperability. Many speakers will extol the next big thing in healthcare system connectivity and large EHR vendors will swear their size fits all and with the wave of video demo, interoperability is declared cured. Long live proprietary solutions, down with system integration and collaboration. Healthcare IT, reborn into the latest vendor initiative, costing billions of dollars and who knows how many thousands of lives.
Physicians’ satisfaction with electronic health record (EHR) systems has declined by nearly 30 percentage points over the last five years, according to a 2015 survey of 940 physicians conducted by the American Medical Association (AMA) and American EHR Partners. The survey found 34 percent of respondents said they were satisfied or very satisfied with their EHR systems, compared with 61 percent of respondents in a similar survey conducted five years ago.
Specifically, the survey found:
42 percent of respondents described their EHR system’s ability to improve efficiency as difficult or very difficult;
43 percent of respondents said they were still addressing productivity challenges related to their EHR system;
54 percent of respondents said their EHR system increased total operating costs; and
72 percent of respondents described their EHR system’s ability to decrease workload as difficult or very difficult.
Whether in the presidential election campaign or at HIMSS, outside of the convention center hype, our abilities are confined by real world facts. Widespread implementation of EHRs have been driven by physician and hospital incentives from the HITECH Act with the laudable goals of improving quality, reducing costs, and engaging patients in their healthcare decisions. All of these goals are dependent on readily available access to patient information.
Whether the access is required by a health professional or a computers’ algorithm generating alerts concerning data, potential adverse events, medication interactions or routine health screenings, healthcare systems have been designed to connect various health data stores. The design and connection of various databases can become the limiting factor for patient safety, efficiency and user experiences in EHR systems.
Healthcare Evolving
Healthcare, and the increasing amount of data being collected to manage the individual, as well as patient populations, is a complex and evolving specialty of medicine. The health information systems used to manage the flow of patient data adds additional complexity with no one system or implementation being the single best solution for any given physician or hospital. Even within the same EHR, implementation decisions impact how healthcare professional workflow and care delivery are restructured to meet the constraints and demands of these data systems.
Physicians and nurses have long uncovered the limitations and barriers EHRs have brought to the trenches of clinical care. Cumbersome interfaces, limited choices for data entry and implementation decisions have increased clinical workloads and added numerous additional warnings which can lead to alert fatigue. Concerns have also been raised for patient safety when critical patient information cannot be located in a timely fashion.
Solving these challenges and developing expansive solutions to improve healthcare delivery, quality and efficiency depends on accessing and connecting data that resides in numerous, often disconnected health data systems located within a single office or spanning across geographically distributed care locations including patients’ homes. With changes in reimbursement from a pay for procedure to a pay for performance model, an understanding of technical solutions and their implementation impacts quality, finances, engagement and patient satisfaction.
Guest post by Khomushka Andrey, project coordinator, Sciencesoft.
Health professionals will hardly ever love documenting. By making tedious tasks easier and eliminating paperwork, medical apps spare time for doctors to focus on their patients more. However, physicians would rather use paper charts and sticky notes than try to figure out what goes wrong with the software.
The reason why mHealth for medical practices, clinics, hospitals and other care organizations might stay unused is that developers tend to build monolithic mobile copies of medical desktop solutions, trying to adapt the complex functionality to smaller screens. Off-the-shelf software vendors generally stick to this large-screen approach, as their goal is to cover the needs of as many customers as possible.
According to Healthcare IT News and the AMA (American Medical Association), however, physicians welcome a more customized approach. “Physicians have found that most EHRs lack usability and interoperability as necessary features for supporting high-quality patient care,” says James L. Madara, MD, CEO of the AMA.
So thinks the AAPS (Association of American Physicians and Surgeons), which represents the end users of such apps. Executive director Jane M. Orient, MD, states that “The costly, clunky systems the government demands are worsening the problems and even driving some software experts back to paper.” And just to emphasize it, according to Healthcare IT News, 80 percent out of 571 physicians surveyed feel that EHRs impede patient care and almost half claim that patient safety is at risk.
Guest post by Mark Ott, vice president of product, RoundingWell.
Mark Ott
As 2016 unfolds, the move from fee-for-service to value-based care is entering a more advanced stage. As the process evolves, priorities for healthcare providers of resources, teams and tools becomes more convoluted. To keep on track, both for healthcare organizations and CMS changes, providers should keep in mind the following:
The care management/coordination record rises in importance, especially as team-based care models expand
Some call it a care management medical record and others call it a care coordination record. Regardless of the term, the concept is essentially the same. EHRs are basically encounter management systems, but as care expands beyond the in-person encounter, capturing and tracking what happens between patient visits will be of utmost importance. In addition, enabling care teams to stay on the same page about a patient’s care plan, track action steps, and reduce the friction of working together will be crucial to succeeding in a value-based world. Expect to see the Care Management Record concept start catching fire in 2016.
Demand will increase for consumer-grade user experiences in healthcare enterprise software
For so long, clinicians on the frontlines of care delivery have had to struggle with software that’s hard to use, difficult and downright frustrating. The biggest culprit for poor user experiences in healthcare software has to do with the enterprise purchasing process. Vendors build for buyers, like the C-suite, who aren’t also the end users. If the end user and the buyer were the same, you’d see healthcare software vendors value user experience like what we see in other B2B industries, not to mention B2C industries. Regardless, in 2016 we will see more buyers value products with consumer-grade user experiences. Much of this has to do with end users’ reluctance and sometimes outright resistance to adopting technology in their worklife. Clinicians often get a bad wrap for being technology averse. But in reality, it’s not that they’re averse to technology; it’s that they’re averse to bad technology.
Integrating wearables and their data into care delivery processes will remain a niche activity
The enthusiasm around wearables, trackers and remote monitoring is exciting and there is enormous potential for device data to impact the delivery of care in ways that benefit both patient and provider. But the technology hasn’t caught up with the promise of what they can be, and that won’t change in 2016. Not only is the technology not yet able to deliver, but the incentives and processes to support wide-scale deployment are not in place yet. Though all signs point to wearables becoming an integral part of delivery of care, this won’t happen next year.
Thanks to remarkable innovations in healthcare technology, the days of having to wait for a doctor’s appointment and travel to their surgical practice are becoming a thing of the past. We have now entered an age where, instead of patients having to attend at a medical practice, their doctor can now visit them virtually in hologram form. It sounds like something out of the realms of science fiction, but this is now a wonderful reality. Welcome to the healthcare of the future!
Home Healthcare Adaptations constructed this infographic, which takes a look at the route that healthcare is set to take in the foreseeable future. The virtual healthcare method outlined above has the potential to create vast savings for the healthcare industry, both financially and in terms of human hours. Indeed, an average reduction of just five minutes in ambulatory visits could possibly free up $58 million in physician capacity.
This new virtual healthcare world could prove highly beneficial both for doctors and the general public. Healthcare professionals can save time on treating patients, which in turn enables them to treat a larger number of patients, and it also reduces the need for them to physically visit a patient’s home, as they can now do so through a hologram from their surgical practice. For patients, it means they don’t have to spend time travelling to a surgical practice and, with doctors able to tend to patients more quickly, it will also reduce patients’ waiting time to receive vital treatment.
Despite these obvious benefits, there is still some resistance to virtual healthcare, with a viewpoint that it will be costly to implement and will require medical professionals to become licencsed telemedicine practitioners. However, as the world becomes more technologically advanced in all aspects, it is hard to see these wonderful new medical practices not becoming regularly used in the near future.
Guest post by Adam Hawkins, vice president client services, CynergisTek.
Adam Hawkins
HIMSS 2016 is right around the corner, and I’m sure everyone is excited about the prospects of conferencing in Las Vegas. This location certainly has a lot going on to keep everyone busy, on and off the exhibit floor. There should be many new healthcare technology players to see and learn about, and it is always interesting to visit the innovation area. Hopefully, we’ll get to hear what folks like KLAS, HIMSS Analytics and other research organizations are working on in 2016 as well.
For instance, KLAS is continuing its work toward including security vendors as its own category, and has a new study underway to look at service providers in this space. That study won’t be completed in time for HIMSS, but they should be able to preview what they hope to accomplish with the study and what its report will include. I think it will be an important read for everyone in our industry.
Interoperability is a huge area of concentration in healthcare at the moment with the Office of the National Coordinator, Health & Human Services and HIMSS all very much involved in this discussion. There are sure to be several presentations on this and related topics. Hopefully we will hear how security and privacy will be addressed, as they are critical components of making many of our health initiatives successful and rely heavily on interoperability for success.
Guest post by Linda Lockwood, solutions director and service line owner, health solutions, CTG.
Linda Lockwood
With HIMSS 2016 fast approaching, the hunt for the perfect Population Health tool will be underway. Whether you’re a HIMSS veteran or a first-time attendee, expect to be caught in a jungle of vendors, each promising the latest and greatest Population Health tools.
HIMSS seems to grow each year, and with so many vendors, solutions and offerings, and the buzz happening during the event, it can be a challenge to carefully evaluate Population Health tools to help inform a decision.
HIMSS can make you excited for the future of your organization, but can also be overwhelming with so many Population Health options to consider. These six tips can help you separate fact from fiction and select a tool that best meets the population health needs of your organization:
Identify organizational goals for population health and match your tool choice to those goals: It’s important to understand what your organizational goals are, as they will drive the selection of tools. If you have not entered into risk bearing agreements, but want to be prepared, perhaps you may want to start off with a tool that supports development of registries and profiles physician performance. You will also want to identify your high risk, high cost patients, and be sure you have the ability to track this performance over time. This information may be available from your financial systems, but you also will need to have the ability to drill down to the device, and supply level—as well as use of medications and supplies including blood products—to identify opportunities for improvement.
How does joining an ACO impact your decision? If you have plans to join an ACO, your needs may include the ability to perform Care Management and Care Coordination and Patient Engagement. You will want to be sure that there is interoperability between the hospital, physician offices and care managers as well as the payers. Reporting becomes critical with an ACO as certain metrics must be reported on a regular basis. As you evaluate tools, ask if they have pre-build reports that include some of the standard measures that a MSSP requires, as well as CMS.
Think about mergers and acquisitions: If you are in the process of a merger or acquiring physicians, you must ensure whatever tool you include has the ability to aggregate data from multiple EHRs and formulate a plan to support interoperability for sharing and exchanging key data. If you are self insured, your organization will have access to data about your population. If you are focusing on wellness and prevention, you will want tools to support patient engagement, health and wellness. Alternately, if have high risk patients, you require Population Health tools to support care coordination, outreach, pharmacy and lab adherence and wellness reminders.
Make data quality a priority: The ability to have accurate, reliable data is crucial with any Population Health or reporting tool. If a data governance system is in place, it’s important to understand what source data you will need to populate the tool. Be sure you know where key data is entered in the system and the common values for that data. In tandem with this, the organization should identify data stewards and business owners. Data governance must have organization-wide commitment, and business owners who are actively engaged.
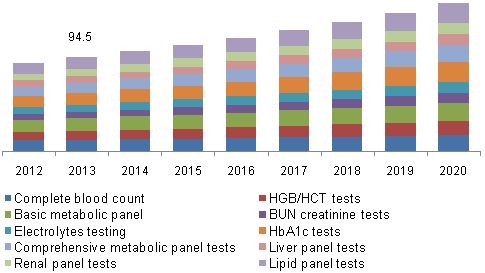
With the global clinical laboratory market slated to grow at an estimated CAGR of 6.8 percent between 2014 and 2020, the importance of clinical testing cannot be underestimated. The development of advanced lab testing techniques is expected to drive the market to a record high of USD 148.8 billion by 2020, making dynamic imaging experiments – the backbone of life science research – a focal point of 21st century R&D.
Dynamic imaging is a central component of lab testing, galvanizing a world of minute cell-level detail into actionable insights. However, for the average life scientist, the need to make hard trade-offs between price, focus and data management can limit the nature and kind of testing that can be done, and hence, the results that are reaped. Whether the research is on something as common as the place of springtime allergies in pediatrics, or as fresh as the role of epigenetic tags in inheritance, life scientists need a camera system that allows them access to minute data, sensitive performance and excellent data management and interpretation. Two imaging options available to them are Charged-Coupled Device (CCD) and scientific Complementary Metal–Oxide–Semiconductor (sCMOS) cameras. But which scientific-grade camera system works in which situation?
CCD vs. sCMOS – Choosing the correct scientific-grade camera
CCD and CMOS technologies both originated in the late 60s – early 70s, each designed to perform the same basic function: capturing, gathering and converting light to produce electronic signals. CCDC cameras dominated the scientific imaging market from the start, as first-generation sCMOS sensors struggled to fabricate quality data. Recent enhancements in sensor design, however, have closed the gap between CCD and sCMOS, allowing the latter to gain ground in life science circles.
Everybody knows that the US healthcare system is in trouble. Issues ranging from cost, to quality and access of care are rampant and only getting worse. On a macro level The Affordable Care Act (ACA) has solved some of the previous access issues, but has added tremendous cost within the system, and at the same time it has not solved the quality issues that exists.
Research suggests that the cost situation is becoming increasingly worse, which is causing firms to scramble for viability. Waves of cost cutting efforts have led payers and providers to capture some, but not nearly enough of the costs necessary for long-term survival.
There are two main cost challenges that both healthcare payers and providers share:
Wildly inefficient operating models and processes. The Harvard School of Public Health projects that of the $2.8 trillion the US spends on healthcare each year, 30 percent or $840 billion may be wasted. For organizations that function on small operating margins, this alone represents the boundary between success and failure.
Large stranded infrastructure and costs combined with declining revenues – The ratio of hospital expense vs. revenue has increased from just under 15 percent in 2011 to nearly 30 percent in 2014 with 25 percent of hospitals reporting an operating loss. For nearly 49 million enrollees in Medicare, hospitals receive only 88 cents for every dollar with lower reimbursement rates predicted in the future.
These pressures have led organizations to make hasty decisions about how to fundamentally solve the problem. Merger and acquisition activity among both payers and providers is at an all-time high, and the ACA appears to have been the catalyst for this M&A activity. Since its enactment, hospitals started merging with competitors at unprecedented rates. In 2009, pre-ACA, there were 52 announced transactions involving 80 hospitals. That number more than doubled by 2012, with 107 announced transactions involving 244 hospitals. The M&A frenzy among healthcare payers has also increased with Anthem’s announcement to acquire Cigna, and Aetna’s acquisition of Humana. Both of these were announced last year and are two of the largest payer M&A deals in history.