In this, the day and age of the global coronavirus outbreak, the job of the medical translator and interpreter has never been more relevant. Resolving this global crisis involves a great deal of research and analysis, much of it in the form of clinical trials. All of the requisite research and analysis must not only be reported and published but accurately documented as well. Once all of the research from the clinical trials has been completed, the information must be made readily available.
The document translation must be completed by certified medical translators and disseminated globally in order for the research to be relevant and helpful. This is an absolutely crucial role during any medically related global crisis but the medical translation of the clinical trial documentation will ultimately be the key to bringing the COVID-19 global pandemic to a successful conclusion before it can get any worse for the people of the world.
In tandem with the need for medical translation is the localization of clinical trials, which requires additional paperwork that the medical translator must make accessible to the world.
Document Requirements for Domestic and International
According to the National Institute of Health, “One of the most common inspection findings in investigator site inspections is lack of reliable, accurate and adequate source documentation. This also happens to be the most common pitfall identified during sponsor audits. The importance of good documentation practice needs to be emphasized to investigator sites to ensure that the study results are built on the foundation of credible and valid data.”
One of the biggest concerns during the current global medical crisis is that many of the clinical trials will not be properly published at all. Of those that are, many will suffer due to the improper documentation and document recordings, and all this before medical document translation begins. Among the biggest culprits of under-reporting, clinical trials were many academic institutions where certified medical translators should be readily available, and clinical trial document requirements should not be a challenge.
A study from the US Food and Drug Administration which is responsible for the oversight and investigation of Clinical Trials in the United States, inadequate documentation records were one of the top causes of clinical trials being brought into question or having them dismissed completely.
Clinical Trial Audits were most commonly required according to the FDA because of the following reasons:
failure to follow the investigational plan (34%)
inadequately informed consent form (28%)
inadequate/inaccurate records (27%)
The amount of documentation required to conduct a clinical trial is overwhelming on the best of days. Every one of the documents is absolutely relevant to the successful conclusion of the clinical trials being conducted by medical researchers.
This is especially true in terms of the current global Covid-19 pandemic. In terms of global clinical trials, translation services should work in support of the global effort, though this also requires that all of the documentation is in order, to begin with. Further, it relies on medical researchers working with a certified medical translation agency that also has the capacity to integrate and implement successful localization strategies to ensure the accuracy of the medical translations before they are distributed globally.
We all know that getting a good night’s sleep is highly beneficial to our bodies. It makes us feel happier, enhances the way our body functions, improves our productivity and concentration, and even decreases the risk of health conditions, such as heart disease and strokes.
A healthy amount of sleep is said to be between seven to eight hours every night. Unfortunately, during this modern day and age, many of us are losing out on essential hours of sleep and the quality of our sleep has seen a massive decline. To improve the way we sleep, many companies are doing their best to develop sleep aid technologies.
Alongside taking the steps to change our sleeping habits for the better, using these technologies could work to our advantage by increasing the amount of sleep we get and enhancing our sleep quality. Today, we will be taking a look at how technology is revolutionizing the sleep industry and some of the technology that is available to us today.
Healthcare has always been one of the largest industries out there, and it certainly won’t be going anywhere anytime soon. To break into this field, a healthcare degree is a must. Here are just five great reasons to study for a healthcare administration degree.
Making a Positive Impact
Retail, hospitality and many other jobs such as this do not provide the moral and emotional benefits that a healthcare administration role can bring. For those with a caring nature who perhaps aren’t suitable for the front lines of healthcare, administrators can still make a huge difference in healthcare systems and go home feeling fulfilled every day. Some of the ways in which you can make a positive impact include:
Influencing future healthcare policies (see below)
Helping others
Improving public education
Contributing to medical investigations and studies
If you are looking for a worthwhile and fulfilling career, healthcare administration may be for you.
Positive Outlook and Salary
Healthcare facilities are always expanding, and with the breakthrough in technology and medicines, people are living for far longer and with much more complex conditions and diseases than ever before. This means that no matter what route you go down in healthcare, you will always be needed.
In fact, in the next four years, the projected growth of healthcare administration and management is 17%, which is larger than many other occupations. Going into healthcare administration in starting roles can see you earning around $29,000 a year, but this can soon increase as you climb the career ladder and get into managerial roles within healthcare administration.
Healthcare is a growing field and one which will provide you with great pay and a positive career outlook.
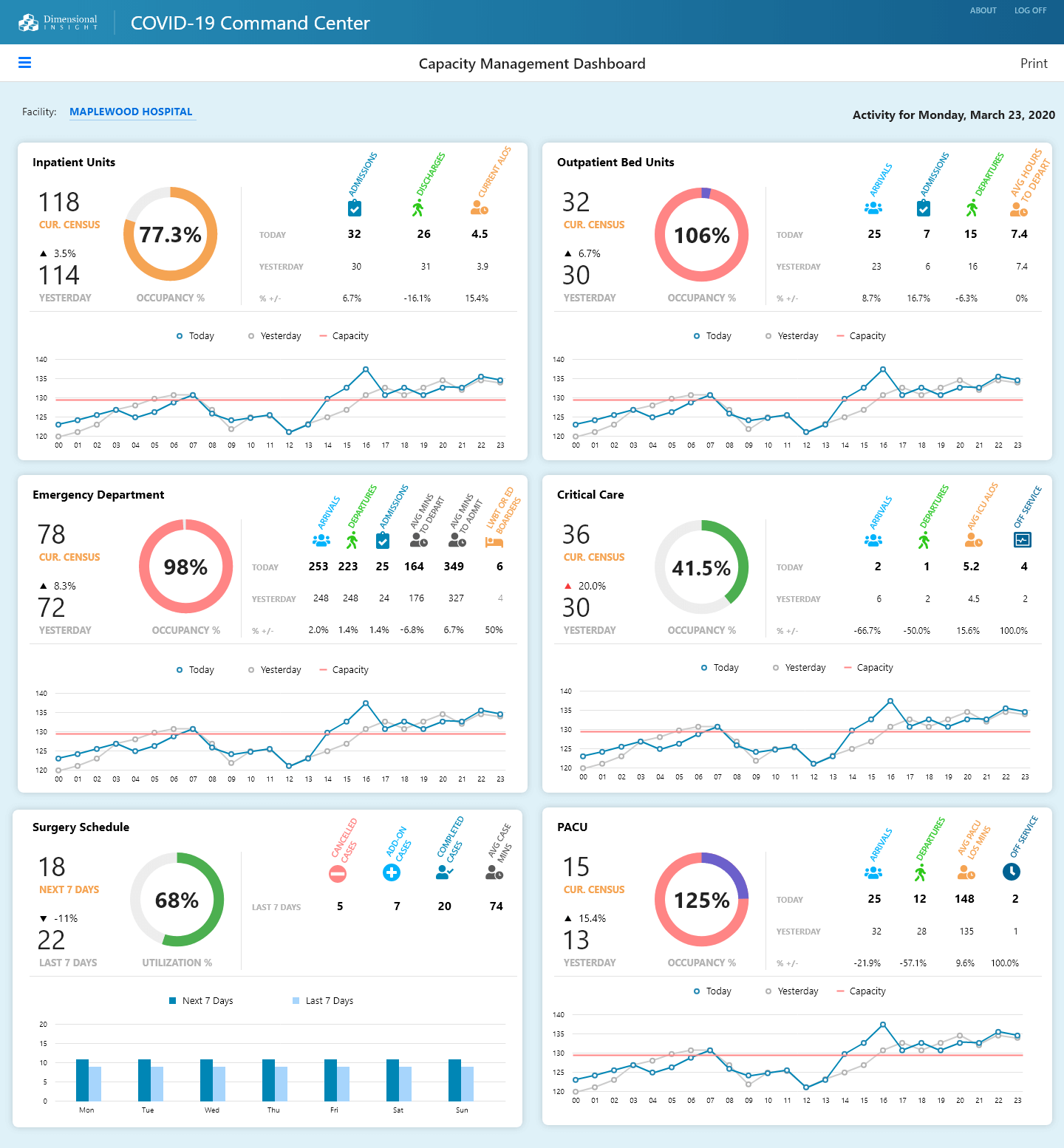
Dimensional Insight, maker of Diver Platform, the 2020 Best in KLAS healthcare business intelligence/analytics platform, today announced it is providing a complimentary* COVID-19 toolkit to healthcare providers.
This kit will provide critical measures or KPIs that hospitals and health systems need to track to better manage their COVID-19 patients, as well as the rest of their patient population. It will also include a capacity management dashboard that displays these current measures in an easy to understand format. In addition, the toolkit will include the logic to implement COVID-19 specific measures based on criteria provided by the CDC. This will result in better, more informed decisions in order to improve patient outcomes.
“As healthcare providers mobilize in their response to the COVID-19 pandemic, their data is an important guide in helping them understand where their resources are being used and what their capacity is as new patients come in,” says Fred Powers, CEO and co-founder of Dimensional Insight. “We are glad to share our expertise with healthcare organizations and provide this toolkit to them when it’s needed most.”
Some of the measures that the new COVID-19 toolkit will contain are related to:
COVID-19 specific (Confirmed COVID-19 cases, Potential COVID-19 cases, COVID-19 ALOS)
Inpatient Units (Census, Occupancy %, Admissions, Discharges, ALOS)
Outpatient Units (Census, Occupancy %, Arrivals, Admissions, Departures, Average Hours to Depart)
Emergency Department (Census, Occupancy %, Arrivals, Departures, Admissions, Average Minutes, LWBT)
Critical Care (Census, Occupancy %, Arrivals, Departures, Average ICU ALOS, Off service)
Surgery Schedule (Utilization %, Cancelled Cases, Add-On Cases, Completed Cases, Average Case Minutes)
PACU (Census, Occupancy %, Arrivals, Departures, Average PACU LOS Minutes, Off service)
Response from Oliver Lignell, vice president, virtual health, AVIA
Providers have a new tool to help them combat COVID-19: digital. Health systems are proactively leveraging digital assets to help triage, navigate, and treat cases in ways that address concerns and also reduce the spread of the virus to other patients and providers.
Virtual assistants and chatbots can help consumers explore symptoms, accurately triage their needs, and navigate them to the appropriate site of care. These solutions can both reduce consumer worries and potentially inappropriate use of EDs and urgent care clinics.
Virtual visits are another critical digital tool because they allow patients to complete a visit from the safety and comfort of their home without exposing them to crowded and potentially infectious clinical locations and, just as importantly, reduces wait times and crowds at in-person care sites.
Asynchronous virtual visits (store and forward, text/chat) can also be an important (and low-cost) solution. Consumers can initiate a low acuity visit on-demand, when convenient, ensuring their concerns are addressed when desired – with the added benefit of decreasing wait times, creating a more efficient patient flow, and freeing up provider capacity. Such solutions further reduce the pressure on health systems while improving the responsiveness to patients.
Response from Andrea Tait, vice president of Client Value, Orion Health
Digital tools can play a key role as healthcare providers across the globe struggle to maintain the health of their workforce and the capacity of their organizations. Pandemic response is best supported through triaging, testing and treating the affected. Tools like public-facing screeners, pandemic information sites and chatbots can help evaluate millions of people with little to no clinician support.
By triaging individuals, tools like remote patient monitoring and telehealth can be used to monitor patients from their homes and assure others that sheltering in place is sufficient. Remote monitoring tools allow clinicians to monitor more patients and make decisions about who may require testing. Designated testing sites minimize the need for direct interaction between healthcare providers and patients, preserving both the health and capacity of health service providers.
Integrated care pathways and telehealth tools can help clinicians treat more patients at home and discharge those in hospitals who may be safer receiving treatment for other conditions remotely, all while minimizing their own risk. Home and community delivered care is an increasingly essential component of healthcare system sustainability. Now, more than ever, these tools and strategies are fundamental to the future of the healthcare system.
Digital solutions can be employed in seemingly non-traditional ways to both prepare and respond to the impact of the coronavirus. For healthcare organizations, traditional pre-access telephone dialing metrics can be modified. Hospital registration staff, in addition to financial guidance and scheduling, can screen patients for COVID-19 and obtain additional clinical information in advance of arrival.
By identifying potentially infected patients, even before they enter the hospital, hospitals and clinics are able to communicate effectively within the facility and plan for appropriate patient care, monitor and manage potential for healthcare personnel COVID-19 exposure, and inhibit the spread of the disease both within the facility and community.
Equally important and sometimes forgotten, back-end services provided by both hospital staff and revenue cycle vendors yields the same patient communication opportunities. Discharged patient follow up and screening post-discharge keeps the patients connected and engaged with the hospital as well as preserves an open communication line between the hospital and discharged patient.
Response from Matthew A. Michela, president and CEO, Life Image
The coronavirus has manifested the importance of digital solutions and interoperability in a heightened way. The lack of digital connections to community referral sites will impact the safety of patients and healthcare staff. It is imperative during this public health crisis that attending healthcare workers have as much relevant clinical data in advance as possible through digital connections.
Unfortunately, many healthcare organizations are still deploying outdated technology, such as imaging CDs, and the last thing a provider or hospital should want is a patient who is symptomatic or potentially a carrier of a virus to show up with a CD in hand. This presents a problem on multiple levels, from the lack of care coordination to the risk of disease spread.
The technology is available and many large health systems are set up to support digital exchange, so they need to mandate protocols to exchange information in this manner. In the same way that the public is asked to wash their hands and frontline workers are urged to wear masks, healthcare professionals should insist that medical data is received digitally for fast, efficient care.
As we face the COVID-19 pandemic, it is important for hospital organizations to ensure information is delivered in real time, accurately, and highly customized to the intended audience (patients, visitors, clinicians, etc.). It can be beneficial for hospitals to automatically deliver COVID-19 patient education videos tailored for each patient’s demographics, language, and clinical circumstances.
This also includes educational content and notifications (visitor restrictions, live updates, social distancing practices, etc.) on digital signage locations in public areas throughout hospitals. That content can be delivered in notifications or in response to Real-Time Location System (RTLS) triggers (for example, if a clinician enters the room, the patient’s TV will display hand washing reminders).
RTLS integration can also track and report staff entries into patient rooms so hospital leaders have real-time data about potential exposures, isolation violations, or interactions with non-approved staff. Interactive surveys with branch logic can help guide patients to provide vital feedback and report any hand hygiene breaches. Digital meal ordering, service requests, and virtual visits decrease human-to-human contact while helping patients get the food, care, services, and items they need. Live streaming (either soothing content like an aquarium or information sources) can also provide distraction therapy and education for patients in isolation.
The American Hospital Association (AHA) recently determined that 75% of senior hospital executives endorsed the importance of digital innovation. This is incredible progress for the industry, but there are still key areas within hospitals that need to embrace the new technologies available, for both the health of the hospital and its patients.
One of the most underserved departments when it comes to innovation is the Neonatal Intensive Care Unit (NICU). The lack of investment might come from the assumption that it’s too small of a population, but these infants are one of the most expensive patients in a hospital, with some preterm infants staying in the NICU over 100 days.
Nutrition: The Overlooked Piece in Preterm Infant Health
More than 380,000 babies in the United States are born preterm annually, and according to the CDC, in 2018, one in 10 babies was born too early (before 37 weeks of pregnancy). Today, we can survive infants as early as 22 weeks gestational age.
Preterm infants require round-the-clock care in the NICU, including monitoring of their hearts, lungs and temperature. As survival rates for extremely preterm infants improve, attention is now being focused on improving the quality of survival. Optimal nutrition early in life can positively impact not only physical growth, but neurological development, as well.
However, nutrition is rarely taught in medical school and expertise is limited to dietitians, where present, or a clinical researcher who focuses on nutrition. Optimizing feeding and nutrition management in the NICU remains a major challenge for clinicians.
Implementing a standardized feeding strategy has been shown to improve growth outcomes in addition to reducing adverse events, however most NICUs are still using paper-based feeding protocols and require dieticians to make manual calculations using pen, paper and calculator.
This manual process has been the standard practice for decades. Not only does this provide room for error, it creates more work for clinical care teams and is a drain on hospital resources. While technology in support of life saving measures is rampant in the NICU, the utilization of software has been limited to the implementation of electronic medical record systems, such as Epic and Cerner. Investments in technological innovations have not extended to addressing feeding and nutritional support for the tiniest, most vulnerable patients.
By Priya Sabharwal, practice leader, network operations, HGS.
Priya Sabharwal
Imagine a scenario: A patient looking for a new doctor searches her insurer’s online network directory to find a provider her plan will cover. She selects what seems to be the perfect doctor based on her criteria, which could include gender, office location, languages spoken or other qualifications, in addition to being in-network with her health plan.
But there’s a plot twist: The patient eventually learns the doctor she found is not, in fact, the right option for her – but it took her scheduling and arriving at the appointment for her to realize this. It turned out the entry in her insurer’s directory was outdated, and her doctor had moved offices.
This scenario is hardly out of the ordinary. A 2019 Health and Human Services survey uncovered errors in half of the listings in Medicare plans alone. These significant inaccuracies cause issues not just for patients, but for payers and providers, too:
Poor directories are more than just an inconvenience for a member; they also impede their access to necessary care, and can create unexpected medical costs.
A typical health plan is already regularly contacting providers’ offices for many different types of data requests. When they also call to verify provider directory requests, it can create added pain for both sides of the equation. On the payer side, it can create provider abrasion, which could influence whether the provider keeps doing business with that payer. On the provider side, receptionists and office managers are pulled away from their higher-level tasks whenever they stop to answer the phone, leading to short-term frustration and, potentially, burnout.
Payers risk incurring stiff fines and penalties from federal and financial entities, and/or member lawsuits. For example, as of 2016, CMS regulations now permit the agency to fine health plans up to $25,000 per Medicare beneficiary for errors in Medicare Advantage plan directories, and up to $100 per beneficiary for mistakes in plans sold on the Affordable Care Act exchanges.
Poor provider data management hinders effective patient-provider matching, patient satisfaction, and demand conversion through call centers.
If a health plan’s website does not contain thorough, accurate provider information, or reflect correct provider availability, potential patients may go back to the drawing board and select a provider from a different organization.
A lack of complete and reliable provider data about specialists leads to misdirected referrals, and acts as a barrier to patient retention within networks.
So what are some steps payers and health plans can take to create a solid provider data foundation? It starts with fundamentally changing the way we think about, use, enter and maintain data.
Many people call retirement the golden years, and they look forward to it for decades. However, those who make the wrong decisions before and during retirement could find that it’s not as pleasant as they anticipated. Here are some useful tips to help you start your retirement right and increase your happiness and health.
1. Decide When to Start Getting Social Security Benefits
When you retire, you may not want to start withdrawing your Social Security benefits. People who retire early could have to wait to apply for Social Security benefits, and others might not receive the full benefit. According to the Social Security Administration, you can start getting Social Security benefits when you turn 62, but you’ll get about 30% less every month. If you wait and use your retirement savings alone or continue to work for a while, your benefits will increase.
 Dimensional Insight, maker of
Dimensional Insight, maker of 


