Elsevier, a global leader in information analytics specializing in science and health, today introduces Veridata EDC, a secure, compliant and user-friendly platform to capture patient data for clinical research.
Veridata EDC is a next-generation version of Elsevier’s MACRO, a solution that has been proven in commercial and not-for-profit clinical research for more than 20 years.
To assist researchers working to develop vaccines and other therapies for COVID-19, Elsevier has pledged to make Veridata EDC available for free. Interested clinical researchers can contact Elsevier customer support via e-mail at covid19@elsevier.com and apply for a demo account. Following the necessary compliance training, they will receive a free 12-month license.
“As researchers around the globe unite to fight COVID-19, they urgently need ways to streamline data collection and facilitate workflows in their studies,” said Olaf Lodbrok, Senior Vice President for Precision Medicine, Global Clinical Solutions, Elsevier. “Veridata EDC is a platform that optimizes data to help them find untold insights faster and more easily.
“COVID-19 is perhaps the biggest challenge in healthcare today. Elsevier is proud to offer clinical researchers a free solution that can transform data points into knowledge to improve clinician collaboration and hopefully patient outcomes.”
Veridata EDC provides clinical researchers with secure and compliant electronic data capture to ensure that the rights, safety and well-being of clinical trial participants are protected. Its intuitive user interface means researchers can quickly input, monitor and run reports to collect accurate and reliable subject data for analysis.
“Veridata EDC breaks down the barriers to research for COVID-19 and beyond. We believe the long legacy of Veridata EDC, combined with its sophisticated functionality, provides the research community with a solution they can trust to further medical discovery,” said Dr. John Danaher, president of global clinical solutions, Elsevier. “Along with Elsevier’s Novel Coronavirus Information Center, our one-stop access to the latest medical and scientific information on coronavirus from across Elsevier’s journals and clinical resources, we are pleased to be a company helping clinicians and clinical researchers on the front lines of fighting this outbreak.”
The HIPAA waiver issued for telemedicine during COVID-19 is a game-changer for physicians now that CMS says virtual visits are reimbursable.
And now, telehealth is emerging as an effective and sustainable solution for precaution, prevention, and treatment to stem the spread of COVIS-19. But what do the new HIPAA waiver and CMS rule about telemedicine during COVID-19 mean?
According to Dr. Neil Baum, chief medical advisor at Vanguard Communications, professor of Clinical Urology at Tulane Medical School, and in clinical practice for 40+ years, the glass is half full.
“Telemedicine is a great opportunity for us to fill our glass and engage our patients in a way we never have before. We’re still able to practice good medicine without having to be face to face or touching a patient,” says Dr. Baum.
Telehealth is bridging the gap between people, physicians, and health systems, enabling everyone, primarily symptomatic patients, to stay at home and communicate with physicians through virtual channels, helping to reduce the spread of the virus to mass populations and the medical staff on the frontlines.
For healthcare professionals, this news means that CMS now allows providers to be reimbursed for the vast majority of virtual visits using telemedicine during the COVID-19 pandemic. (Only a small number qualified for reimbursements as recently as March 14.)
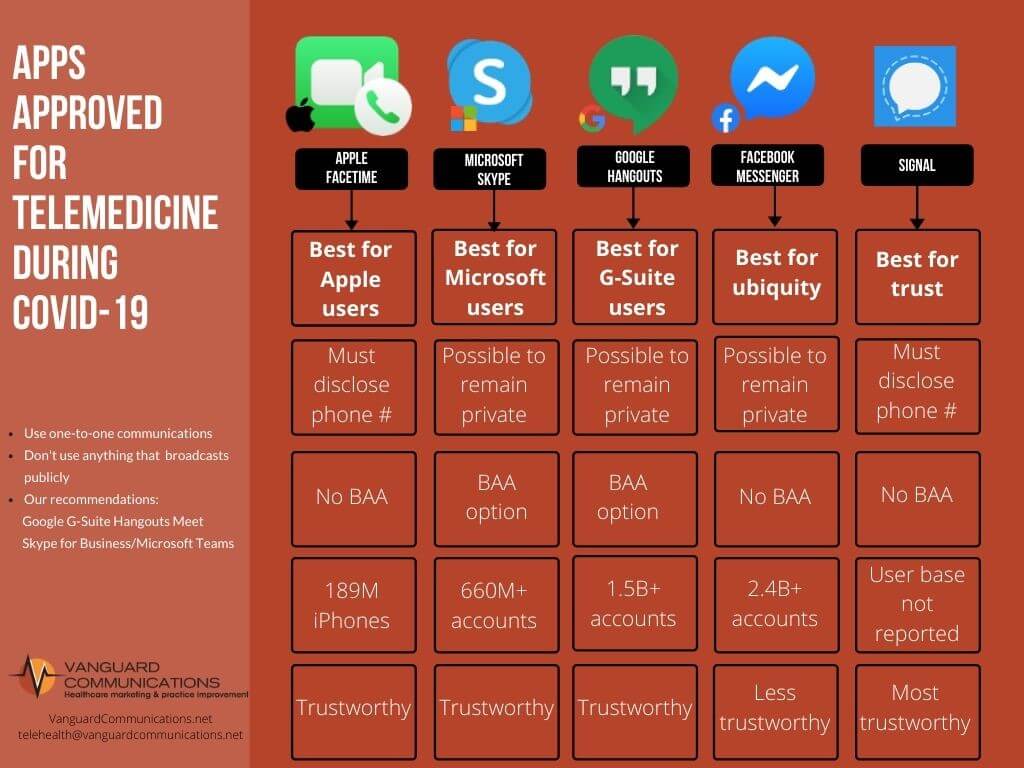
Plus, no special software or extra expense for healthcare-specific hardware and software is needed. The tools are free and easy to use.
Below is a chart of the popular apps approved for telemedicine during COVID-19.
Dr. Baum says telemedicine will go a long way to enhancing a physician’s connection with patients and providing access to care but stresses the importance of documenting virtual visits and video conversations just as you would an in-office appointment.
“If you didn’t document, then you didn’t do it, and then you don’t get paid for it,” says Dr. Baum.
“Every day, heroic nurses, doctors, and other healthcare workers are dedicating long hours to their patients. This means sacrificing time with their families and risking their very lives to care for coronavirus patients,” said CMS Administrator Seema Verma. “Front line healthcare providers need to be able to focus on patient care in the most flexible and innovative ways possible. This unprecedented temporary relaxation in regulation will help the healthcare system deal with patient surges by giving it tools and support to create non-traditional care sites and staff them quickly.”
Other temporary CMS waivers and rule changes dramatically lessen administrative burdens, knowing that front line providers will be operating with high volumes and under extraordinary system stresses.
CMS recently approved hundreds of waiver requests from healthcare providers, state governments, and state hospital associations in the following states: Ohio; Tennessee; Virginia; Missouri; Michigan; New Hampshire; Oregon; California; Washington; Illinois; Iowa; South Dakota; Texas; New Jersey; and North Carolina. With today’s announcement of blanket waivers, other states and providers do not need to apply for these waivers and can begin using the flexibilities immediately.
Administrator Verma added that she applauds the Mar. 23, 2020, pledge by America’s Health Insurance Plans (AHIP) to match CMS’s waivers for Medicare beneficiaries in areas where in-patient capacity is under strain. “It’s a terrific example of public-private partnership and will expand the impact of Medicare’s changes,” Verma said.
CMS’s temporary actions announced today empower local hospitals and healthcare systems to:
Increase Hospital Capacity – CMS Hospitals Without Walls:
CMS will allow communities to take advantage of local ambulatory surgery centers that have canceled elective surgeries, per federal recommendations. Surgery centers can contract with local healthcare systems to provide hospital services, or they can enroll and bill as hospitals during the emergency declaration as long as they are not inconsistent with their State’s Emergency Preparedness or Pandemic Plan. The new flexibilities will also leverage these types of sites to decant services typically provided by hospitals such as cancer procedures, trauma surgeries and other essential surgeries.
CMS will now temporarily permit non-hospital buildings and spaces to be used for patient care and quarantine sites, provided that the location is approved by the State and ensures the safety and comfort of patients and staff. This will expand the capacity of communities to develop a system of care that safely treats patients without COVID-19, and isolate and treat patients with COVID-19.
CMS will also allow hospitals, laboratories, and other entities to perform tests for COVID-19 on people at home and in other community-based settings outside of the hospital. This will both increase access to testing and reduce risks of exposure. The new guidance allows healthcare systems, hospitals, and communities to set up testing sites exclusively for the purpose of identifying COVID-19-positive patients in a safe environment.
In addition, CMS will allow hospital emergency departments to test and screen patients for COVID-19 at drive-through and off-campus test sites.
During the public health emergency, ambulances can transport patients to a wider range of locations when other transportation is not medically appropriate. These destinations include community mental health centers, federally qualified health centers (FQHCs), physician’s offices, urgent care facilities, ambulatory surgery centers, and any locations furnishing dialysis services when an ESRD facility is not available.
Physician-owned hospitals can temporarily increase the number of their licensed beds, operating rooms, and procedure rooms. For example, a physician-owned hospital may temporarily convert observation beds to inpatient beds to accommodate patient surge during the public health emergency.
In addition, hospitals can bill for services provided outside their four walls. Emergency departments of hospitals can use telehealth services to quickly assess patients to determine the most appropriate site of care, freeing emergency space for those that need it most. New rules ensure that patients can be screened at alternate treatment and testing sites which are not subject to the Emergency Medical Labor and Treatment Act (EMTALA) as long as the national emergency remains in force. This will allow hospitals, psychiatric hospitals, and critical access hospitals (CAHs) to screen patients at a location offsite from the hospital’s campus to prevent the spread of COVID-19.
Rapidly Expand the Healthcare Workforce:
Local private practice clinicians and their trained staff may be available for temporary employment since nonessential medical and surgical services are postponed during the public health emergency. CMS’s temporary requirements allow hospitals and healthcare systems to increase their workforce capacity by removing barriers for physicians, nurses, and other clinicians to be readily hired from the local community as well as those licensed from other states without violating Medicare rules.
These healthcare workers can then perform the functions they are qualified and licensed for, while awaiting completion of federal paperwork requirements.
CMS is issuing waivers so that hospitals can use other practitioners, such as physician assistants and nurse practitioners, to the fullest extent possible, in accordance with a state’s emergency preparedness or pandemic plan. These clinicians can perform services such as order tests and medications that may have previously required a physician’s order where this is permitted under state law.
CMS is waiving the requirements that a certified registered nurse anesthetist (CRNA) is under the supervision of a physician. This will allow CRNAs to function to the fullest extent allowed by the state, and free up physicians from the supervisory requirement and expand the capacity of both CRNAs and physicians.
CMS also is issuing a blanket waiver to allow hospitals to provide benefits and support to their medical staffs, such as multiple daily meals, laundry service for personal clothing, or child care services while the physicians and other staff are at the hospital and engaging in activities that benefit the hospital and its patients.
CMS will also allow healthcare providers (clinicians, hospitals and other institutional providers, and suppliers) to enroll in Medicare temporarily to provide care during the public health emergency.
Put Patients over Paperwork:
CMS is temporarily eliminating paperwork requirements and allowing clinicians to spend more time with patients. Medicare will now cover respiratory-related devices and equipment for any medical reason determined by clinicians so that patients can get the care they need; previously Medicare only covered them under certain circumstances.
During the public health emergency, hospitals will not be required to have written policies on processes and visitation of patients who are in COVID-19 isolation. Hospitals will also have more time to provide patients a copy of their medical record.
CMS is providing temporary relief from many audit and reporting requirements so that providers, healthcare facilities, Medicare Advantage health plans, Medicare Part D prescription drug plans, and states can focus on providing needed care to Medicare and Medicaid beneficiaries affected by COVID-19.
This is being done by extending reporting deadlines and suspending documentation requests which would take time away from patient care.
Further Promote Telehealth in Medicare:
Building on prior action to expand reimbursement for telehealth services to Medicare beneficiaries, CMS will now allow for more than 80 additional services to be furnished via telehealth. During the public health emergencies, individuals can use interactive apps with audio and video capabilities to visit with their clinician for an even broader range of services. Providers also can evaluate beneficiaries who have audio phones only.
These temporary changes will ensure that patients have access to physicians and other providers while remaining safely at home.
Providers can bill for telehealth visits at the same rate as in-person visits. Telehealth visits include emergency department visits, initial nursing facility and discharge visits, home visits, and therapy services, which must be provided by a clinician that is allowed to provide telehealth. New as well as established patients now may stay at home and have a telehealth visit with their provider.
CMS is allowing telehealth to fulfill many face-to-face visit requirements for clinicians to see their patients in inpatient rehabilitation facilities, hospice and home health.
CMS is making it clear that clinicians can provide remote patient monitoring services to patients with acute and chronic conditions, and can be provided for patients with only one disease. For example, remote patient monitoring can be used to monitor a patient’s oxygen saturation levels using pulse oximetry.
In addition, CMS is allowing physicians to supervise their clinical staff using virtual technologies when appropriate, instead of requiring in-person presence.
These actions, and earlier CMS actions in response to COVID-19, are part of the ongoing White House Coronavirus Task Force efforts. To keep up with the important work the Task Force is doing in response to COVID-19, visit www.coronavirus.gov. For a complete and updated list of CMS actions, and other information specific to CMS, please visit the Current Emergencies Website.
Visiting nurses are valued for their caring and compassionate nature. Their valuable skillset makes a difference in the well-being of their patients and the lives of patients’ families. However, they face unique challenges amid the coronavirus as patients and staff are concerned about receiving in-home care during this time. Bringing healthcare to the home is no easy task.
As NAHC President William A. Dombi stated, “Home care and hospice nurses, therapists, aides, and other providers who choose to use their lives to serve our country’s aged, disabled, and dying. This noble work deserves our recognition and praise.”
Home health agencies are on the front line amid the coronavirus pandemic. A recent Home Care Association of New York State (HCA-NYS) survey found that nearly half of agencies in the survey said they have experienced patients or family members refusing entry of home care personnel. “Different states and regions are at different stages in surveillance and monitoring,” Roger Noyes, director of communications at HCA-NYS, told Home Health Care News.
“This speaks to some very important educational and outreach needs to reassure patients and to ensure that vital care can be delivered,” Noyes said. In addition to patients’ hesitation to let nurses into their homes for in-person visits, many patients are already quarantined, sheltering in place, or social distancing. And, some patients are denying service because they appreciate their nurses so much that they do not want to risk getting their nurse sick in-person. Concurrently, the nurses themselves might also be wary of conducting in-person visits as they might not have sufficient protective gear and/or fear the risk of infection.
Agencies are implementing telehealth/virtual care to preserve their patients, their staff and their limited supplies. Technology can help agencies’ staff continue what they do – provide compassionate and critical care – and “be present” with their patients as much as possible. With technology, agencies can safely continue the delivery of care during this time and quickly communicate critical updates as needed. The technology helps home healthcare agencies:
Conduct virtual visits with patients to safely ensure continuity of care
Send out critical COVID-19 updates and self-care tips
Send condition-specific messages to improve ongoing adherence
Provide virtual access to their staff which helps nurses address patients’ emerging concerns and also alleviate patients’ loneliness while being socially isolated
With virtual visits, agencies are kept abreast of the realities of the patient’s home environment and their available resources (financial, food, social, etc.). Staff can continue to monitor their patients’ day-to-day situation and individualize the care (and conversation) to the “new normal” for the at-home patient.
The healthcare industry is ripe for disruption and transformation. According to McKinsey & Company, U.S. pharma is “in a state of flux.” Seismic shifts are happening, from significant merger and acquisition (M&A) activity to pharmacy store closures to changes in strategic partnerships between major health insurers and pharmacy benefit managers (PBMs), and the seemingly inevitable entry of Amazon into the market. Moreover, the healthcare ecosystem continues to face challenges as it attempts to comply with regulations like HIPAA and HITECH.
During this period of change, McKinsey’s research establishes three imperatives for healthcare businesses to consider. The first is to pursue business models that deliver a lower total cost of care for consumers and employers. The second involves leveraging data aggregation and big data analytics to generate insights and create value, and the third is to put the consumer at the center of everything by creating innovative ways to bring more consumer-driven insights and actions into the business.
The growth in digital health indicates that many businesses are acting on these imperatives and are finding commercial success. The digital health sector currently is estimated at $86.4 billion and is predicted to grow by almost 30 percent year-over-year through 2025. But with such a vast and complex industry like healthcare, it is challenging to appreciate the realities of digital disruption without drilling down into specific sub-sectors and profiling some of the disruptors that are in the process of altering their landscapes.
Following are some examples of how the “value pool” is shifting in this industry, resulting in cost savings for patients through the elimination of waste.
Pharmacy benefit management value pool shifts by removing inefficiencies
Pharmacy benefit management (PBM) includes third-party administrators for prescription drug programs at insurance companies, businesses, self-insured employers and government health plans. PBMs have a vast market valuation of $368 billion, as of 2018, within the U.S. healthcare system and an expected annual growth forecast of more than 9 percent.
Despite the size of the market, however, many PBMs do not have the technical sophistication to flourish in the digital world, which has given rise to companies such as RxSense. Previously a PBM, RxSense pivoted to meet the real-time needs of customers by providing a business-to-business (B2B) digital platform for the whole PBM industry. Its goal is to bypass problems with legacy PBM systems, including a lack of innovation, inefficiencies, inflexibility and challenges around accuracy and transparency.
The next step beyond digitization for players such as RxSense will be the application of artificial intelligence (AI) and machine learning technologies to further increase administrative efficiency, drive down costs and, ultimately, improve clinical outcomes.
OneBlood, the not-for-profit blood center serving Florida and other parts of the southeastern United States, will soon begin collecting plasma from people who have recovered from the coronavirus so it can be transfused to people with life-threatening coronavirus infection in hopes of aiding their recovery.
The experimental treatment is approved by the FDA to be used on an emergency basis and is called “COVID-19 convalescent plasma.”
People who recover from coronavirus infection have developed antibodies to the virus that remain in the plasma portion of their blood. Transfusing the plasma that contains the antibodies into a person still fighting the virus can provide a boost to the patient’s immune system and potentially help them recover.
OneBlood is working closely with the Florida Department of Health to identify people who have recovered from COVID-19 to be potential donors. In addition to local efforts, OneBlood is also cooperating with the federal government and anticipates participating in a national-level initiative to be able to provide convalescent plasma when and where it is needed.
OneBlood is working quickly to implement the new protocols to meet the FDA criteria for COVID-19 convalescent plasma. OneBlood plans to begin collecting plasma from qualified donors in the coming weeks and also plans to start offering the therapeutic agent to hospitals to treat severely ill coronavirus patients. As one of the largest blood centers in the country, OneBlood already has the technology in place to be able to collect, test and process plasma from donors.
The potential donors will need to meet all the usual screening criteria for blood donation, plus pass additional FDA criteria, including:
COVID-19 convalescent plasma must only be collected from recovered individuals if they are eligible to donate blood
Required testing must be performed and the donation must be found suitable
Prior diagnosis of COVID-19 documented by a laboratory test
Complete resolution of symptoms at least 14 days prior to donation
Have a negative result for COVID-19
Meet all standard FDA blood donation requirements
As with all transfusions, the donor and the patient will need to have compatible blood types
In addition, the recipients of the plasma will also have to meet FDA criteria in order to qualify to receive this therapy for treating life-threatening COVID-19. (Click here for FDA report).
By Brian Kirkendall, vice president of product management, Digi International.
Brian Kirkendall
In 1847, Hungarian physician Ignaz Semmelweis theorized that hand washing could limit the occurrence of puerperal fever among new mothers. But despite the obvious success of his proposal, he faced significant opposition from his colleagues in the medical community, many of whom flatly rejected his theory.
Of course, today more than ever, we’re acutely aware of the importance of Semmelweis’ game-changing understanding of hand washing, and we are tracking it more closely than ever before. Fortunately, our modern healthcare industry is equipped with far more than mere chlorinated lime solutions that our forefathers had in the 19th century. And the Internet of Things (IoT) is stepping in to support healthcare providers with breakthroughs that can enhance our preparedness to fight and prevent infections and mitigate the spread of contagions such as COVID-19.
Can IoT help keep us safe?
The healthcare industry has long been a careful early adopter of lifesaving and life changing innovations, so it comes as no surprise that the IoT has made steady inroads into all types of clinical settings: doctors’ offices, hospitals, clinics, ambulances and more. From patient-connected devices for accurate and vigilant patient care to medical equipment such as pain medication management and hygiene monitoring devices, the IoT is transforming almost every area of healthcare delivery.
The IoT’s compelling combination of compact and low-cost hardware and software creates a far-reaching impact for caregivers and patients alike in the form of improved accuracy, greater efficiency, lower costs, and enhanced health and safety.
Today, one application that’s gaining wide notice is the use of wireless technology to monitor and report on hygiene compliance in the medical industry. The implementation of wireless sensors and flexible gateways are bringing unprecedented precision, including temperature and pressure monitoring in surgical suites, monitoring cryogenic environments or something as routine – but life-saving – as hand hygiene.
A real-life use case: Sanitize your hands
We usually think hospitals are some of the most hygienic places of all. However, given the high traffic of sick people, hospitals that aren’t rigorous and vigilant can be home to greater infectious risks. Due to the number of immunocompromised patients present, hospitals face an ongoing mission-critical challenge to prevent the spread of bacteria and infectious diseases. Long before the COVID-19 global pandemic, the Clean Hands Safe Hands (CHSH) initiative recognized this importance of this issue and promulgated hand washing strategies that use wireless technology to help healthcare institutions promote health and safety.
As simple as it sounds, in a hectic environment like a healthcare facility, simple vigilance in washing hands can be the No. 1 factor in keeping medical workers and patients safer. What a better way to improve hand cleanliness than by providing hospitals with internet-connected hand-sanitizing stations?
As COVID-19 closes in the on U.S., the need for longitudinal health data and interoperability have never been greater. Providers need access to the full picture of every patient they treat, and epidemiologists need to consolidate data from multiple sources to track the spread of the disease and determine where more aggressive containment strategies need to be employed.
For many organizations already overwhelmed, fragmented systems lead to an infrastructure bottleneck, resulting in degraded data quality, gaps in care coordination, medical errors and burdensome workflows. Lack of comprehensive medical data impairs a provider’s ability to know how many people have the virus, the geographical location of confirmed cases, and the effectiveness of treatment.
Even as capacity restrictions force organizations to work without barriers—via drive-thru screenings, make-shift tents or by way of telehealth—real-time access to data can help streamline care management, whether fast tracking admissions or empowering patients at home through online portals.
Here are just five ways data interoperability plays a pivotal role in addressing the epidemic:
Coordination of Care: COVID-19 provides a sobering reminder of just how dire an integrated, scalable and interoperable healthcare infrastructure is. Coordination among first responders, public health officials, labs, acute and post-acute facilities will be critical to efficiently deal with the explosion of cases. Insurers will also be a key player of the care coordination team as to not slow down or hold up prior authorizations and patient discharges. Access to information about hospitalizations and test results among healthcare participants will be vital for enhanced continuity of care across settings and transitions. Real-time data afforded by interoperability bypasses the need for phone calls and faxes, which create delays and information inaccuracies.
Patient Identification: A complete view of one’s medical history can be a matter of life or death in the face of COVID-19. Bringing disparate medical records together into a cohesive story enables those on the frontlines insight into an individual’s pre-existing medical conditions, medications, allergies, etc. to make the most informed decisions under insurmountable circumstances. Patient demographics and data standardization play a huge role. Accurate patient identification ensures data about an individual is correctly linked, updated and shared, for improved clinical decision-making and enhanced care quality and safety. As health officials look to track and predict the spread of the virus. A complete view of the patient population can only be done with a firm understanding of the patient’s identity, and the key relationships the patient has to their next of kin and to their providers of care.

 The healthcare industry is ripe for disruption and transformation. According to McKinsey & Company, U.S. pharma is “
The healthcare industry is ripe for disruption and transformation. According to McKinsey & Company, U.S. pharma is “
