By Aaron Perreira, director of integrated marketing, Kareo.
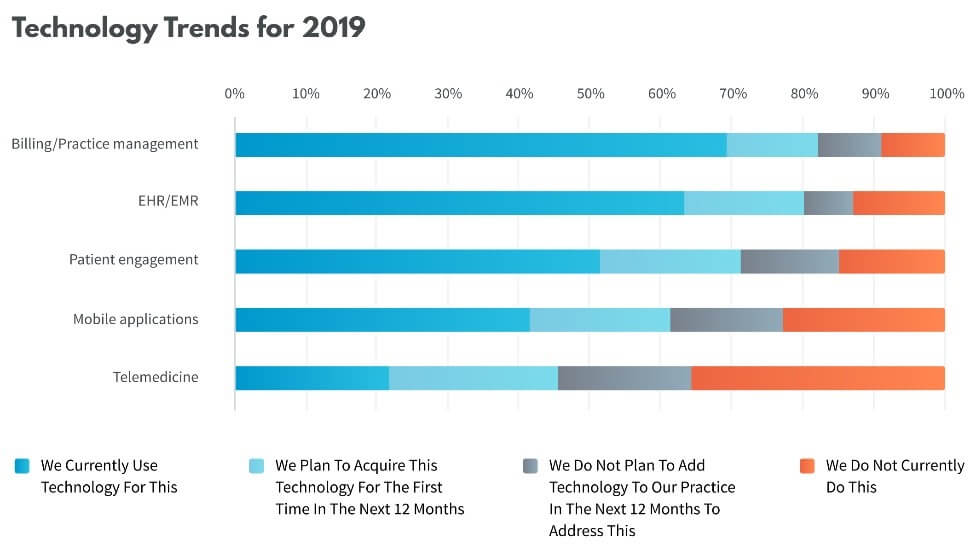
Over 70% of independent medical practices agree that the time demands of electronic health records (EHR) data entry detracts from care delivery. Simultaneously, 69% of independent practices state that integrated technology solutions are needed to improve the efficiency and profitability of their practices. This interesting “love/hate” relationship between independent practitioners and technology was shared in the recent 2019 State of the Independent Practice Industry Report, published by Kareo, a cloud-based medical software company.
The report was based on a nationwide survey designed to uncover the current challenges and expectations of independent practitioners in several areas of their practices, including care delivery, billing, patient engagement and regulatory compliance. Attitudes regarding the role of technology emerged in each of the areas surveyed.
Providers are increasingly reliant on their EHRs to manage their day-to-day clinical operations and maintain regulatory compliance. For many practices, the use of EHRs began when the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 was signed into law by President Obama on February 17, 2009. The HITECH Act was created to motivate the implementation of electronic health records by providing monetary incentives for being able to demonstrate meaningful use of electronic health records.
At that time, the market was flooded with more than 700 EHR vendors looking to capitalize on the EHR gold rush. Many practices adopted EHRs at that time, however since then, as the regulatory standards and consumer requirements for EHR technology continued to evolve, an increasing number of software providers have failed to keep up with technology and have fallen out of the race. This has left many providers tethered to antiquated, ineffective systems. More established practices (in practice for 10 or more years) appear to be more gun shy in that they likely adopted their EHR several years ago and had to suffer through poor implementations of costly but under-performing software that didn’t deliver on the value that was promised.
Despite government mandate, penalties and incentives, only 64% of respondents are currently using an EHR today. This low figure likely represents both the entry of newer practices that haven’t yet implemented their EHR platform and the fact that some practice specialties such as mental health, are more likely to still be using paper-based records and haven’t made the switch to electronic records.
Healthcare data hacking has started occurring pretty often nowadays and most people are not even aware that their data has been stolen. Healthcare organizations are not built in a way they can identify illegal records; hence, they are unable to eliminate them.
The main problem is that people are not aware of healthcare data breach until they are sick and need treatment, which makes it the worst time to deal with problems like this. Breaching of healthcare data leads to losing insurance coverage, mixed up records, wrong diagnosis, medical harm, etc.
Thus, how do you prevent this from happening? Here are here to share some tips that will help you avoid healthcare data hacking.
5 Tips to avoid healthcare data hacking
Lexington Law. Healthcare data theft, along with Identity theft, has become a huge problem in today’s world. In order to stay protected from these things, hiring services like Lexington law can be extremely helpful.
They provide things like free credit report evaluation and attractive discounts for couples, families and active military personnel along with protecting your health care data and identity. You can go over to websites, like Crediful, to read a review about Lexington law before buying.
Do a risk assessment test. In 2003, a rule was passed by HIPAA which stated that healthcare organizations were required to take a risk assessment test. However, there was no penalty if not done, so most organizations did not do it.
Then the HITECH Act passed and it changed the law by making security risk analysis mandatory. Performing security analysis helps in identifying vulnerabilities in the security systems and identifying threats.
Always keep software up to date. Most people neglect software updates as they are busy and do not like the idea of taking the computer system offline for updates, but this is a terrible thing to do, and it puts your data on a huge risk.
The latest version of the software is mainly released to reduce any security risks, and not updating them keeps your devices vulnerable to threats and attacks. You will miss any security patch that comes with the latest updates. Criminals use this to their advantage to steal data from outdated devices. Thus, make sure you always keep all software updated.
By Ken Perez, vice president of healthcare policy, Omnicell, Inc.
Ken Perez
It was such a beautiful, logical vision: The creation of “an electronic circulatory system for health information that nourishes the practice of medicine, research, and public health, making health care professionals better at what they do and the American people healthier,” as David Blumenthal, the National Coordinator for Health Information Technology from 2009 to 2011, wrote in an article on the potential of the HITECH Act’s subsidization of the adoption of EHRs by hospitals and physician practices that appeared in the Dec. 30, 2009, issue of the New England Journal of Medicine.
The HITECH Act was combined with the American Recovery and Reinvestment Act of 2009 (ARRA), an economic stimulus bill created to help the U.S. economy recover from an economic downturn that began in late 2007. The passage of the bill spawned an ambitious vision of an elaborate national health information infrastructure that would enable frictionless, collaborative data sharing primarily through a National Health Information Network (NHIN) that would connect an interlocking web of regional health information organizations (RHIOs) and health information exchanges (HIEs).
It must be emphasized that the NHIN vision was a federal government vision—not one generally shared by the private sector. It was never realized, and the adoption of EHRs by healthcare providers has been described as “a digital revolution gone wrong” and “a bridge to nowhere,” in the 15-page cover article of Fortune magazine’s April issue, entitled “Death by a Thousand Clicks,” by Erika Fry of the magazine and Fred Schulte of Kaiser Health News.
For their report—which has the feel of an exposé — Fry and Schulte interviewed more than 100 physicians, patients, IT experts, administrators, health policy leaders, attorneys, government officials, and representatives from several leading EHR vendors. They employ a combination of poignant vignettes of patients who were harmed by EHR shortcomings — including the experiences of former Vice President Joe Biden’s son Beau and the husband of CMS Administrator Seema Verma — as well as ample facts and figures.
Per Fry and Schulte, the federal government has spent $36 billion to date to subsidize the adoption of EHRs by healthcare providers, and today, 96 percent of non-federal acute care hospitals and 86 percent of physician offices have EHRs.
Despite the significant amount of federal funding and broad adoption of EHRs, they have not fulfilled their potential, as Blumenthal has admitted. The expected “digital dividend” from EHRs has not materialized, or at least its magnitude is much smaller than hoped for. According to Fry and Schulte, EHRs’ general demerits include poor, tedious usability—which adds work and is cited as a major contributing factor to physician burnout — rampant errors that lead to patient safety risks, “upcoding” (bill inflation), lack of interoperability, widespread data blocking, and patients’ inability to access their EHRs. Data silos clearly exist between the 700 federally certified EHRs of widely varying functionality, as well as between provider organizations and other players in the healthcare system. In short, idealism has run into the reality of commercialization.
Fry and Schulte provide no optimistic, Hollywood ending to the article. Industry attempts to promote interoperability are described as fledgling, and their sobering conclusion is that the state of EHRs in the United States is “an unholy mess.”
Have you ever sought medical care from multiple providers for the same condition? Then you probably already know how difficult it can be to coordinate care from one practice or facility to the next. One provider may not necessarily have access to the test results ordered by another provider, and even getting a prescription filled can be a hassle — you have to wait while the pharmacist fills your prescription and hope that he or she doesn’t misread the prescribing doctor’s terrible handwriting.
But all of that is changing; for many patients across the country, it has already changed, thanks to the Health Information Technology for Clinical Health (HITECH) Act of 2009. This law was enacted to encourage the transition to electronic health records (EHRs) in medical practices, hospitals, and other health facilities. Researchers agree that the use of EHRs can have many benefits for providers and patients alike, including improved patient outcomes, reduced costs, streamlined administration, and even improved ability to perform medical research.
What Are EHRs?
An EHR is an electronic record of a patient’s medical history that combines test results, diagnoses, and other data accumulated as the patient moves from one provider to another. Your EHR is meant to be longitudinal in nature, meaning that the record represents a lifetime picture of your health history.
Unlike a medical record, which is maintained by a single provider, an EHR is comprehensive; since it includes information compiled from every provider who works with you, it will offer each provider all of the information necessary to make your next treatment decision. That means no more re-ordering an expensive test you’ve already taken somewhere else, and no more waiting for test results to be faxed over from another doctor’s office.
Advantages of EHRs
Ideally, EHRs will someday travel with you. When all providers have made the transition to using EHR systems such as RevenueXL, you’ll be able to get the same quality of care from providers anywhere in the country. They’ll simply be able to check your EHR for pertinent medical information, and even update it so that your providers back home will be able to adjust your care accordingly. Even if you’re incapacitated, your EHR will ensure that providers around the country will be alerted to your medication list and existing medical conditions.
EHRs should make life easier for everyone involved in your care. You’ll be able to:
Schedule doctor’s appointments online
Ask medical questions via email
Request prescription refills electronically
Access test results whenever you want
Keep track of scheduled appointments
The use of EHRs should streamline the many administrative tasks associated with patient care. EHR system software will prompt your doctor to file necessary Medicare and insurance paperwork, will help them keep track of which best practice guidelines apply to your specific case, and will reduce numerous costs.
With a flourish of congressional shenanigans lifted almost word for word from the teleplay of Netflix’s House of Cards, the HHS-mandated 2014 transition to use of the ICD-10 coding classification was brought to a screeching one year “delay.” We are left, once again, with “at least” another year of collecting healthcare information via ICD-9, an awful but omnipresent healthcare coding system. And more concerning, we are left with the impression that diligent and expensive work to comply with rules in a host of other areas, such as meaningful use of electronic health records, could become abruptly irrelevant. The result of the delay is that not only do we have a significant number of long-time objectors to the change to ICD-10, but they are also joined by a surge of rightfully angry and dubious ‘compliers’ who put in time and investment dollars to meet the deadline. But there are also some additional considerations given the amount of time that has passed as we prepare to make the trip.
Is this trip still worth the aggravation and expense?
The major underlying rationale of moving to ICD-10 remains laudable: to provide greater clarity to our understanding of healthcare practices through the use of better industry standard, diagnosis codes. With more granular, relevant and precise core codes at the foundation, medical quality and effectiveness studies utilizing these codes for analysis and program development were to have benefitted dramatically.
Given that our desire to advance healthcare value and improve outcomes through accountable care practices (‘fee-for-value’) we must acknowledge our dependence on much better information collection for analysis than is possible from ICD-9[1]. Significant questions remain however, as to whether the move to ICD-10, using codes predominantly still entrenched to support fee-for-service billing processes will get us where we want to go. While we can hope the enhanced and detailed nature of ICD-10 might yield greater insight into the real value of our activities, this remains a particularly frail hope in light of the way we use the codes as revenue cycle fuel.
Guest post by Andy Nieto, health IT strategist, DataMotion.
The HITECH Act’s goal of improving clinical outcomes for patients using technology through meaningful use is admirable and quite overdue. However, where the Office of the National Coordinator for Health Information Technology (ONC), and to a much greater extent, electronic health records (EHR), have missed the mark is in the deployment and execution.
The stated goal of meaningful use Stage 1 (MU1) was to deploy, integrate and use EHRs to gather and document “structured and coded” healthcare data. Rather than take ONC’s directives as a framework to improve provider care tools, they viewed it as a “minimum requirement” and missed the spirit of the initiative. EHRs remain cumbersome, challenging and inefficient.
Providers now spend more time clicking boxes and typing than they do speaking to their patients. To make matters worse, the data gathered is maintained in the EHR’s “unique” way, making exchange and interaction challenging and interfaces costly.
 Providers are increasingly reliant on their EHRs to manage their day-to-day clinical operations and maintain regulatory compliance. For many practices, the use of EHRs began when the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 was signed into law by President Obama on February 17, 2009. The HITECH Act was created to motivate the implementation of electronic health records by providing monetary incentives for being able to demonstrate meaningful use of electronic health records.
Providers are increasingly reliant on their EHRs to manage their day-to-day clinical operations and maintain regulatory compliance. For many practices, the use of EHRs began when the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 was signed into law by President Obama on February 17, 2009. The HITECH Act was created to motivate the implementation of electronic health records by providing monetary incentives for being able to demonstrate meaningful use of electronic health records. Healthcare data hacking has started occurring pretty often nowadays and most people are not even aware that their data has been stolen. Healthcare organizations are not built in a way they can identify illegal records; hence, they are unable to eliminate them.
Healthcare data hacking has started occurring pretty often nowadays and most people are not even aware that their data has been stolen. Healthcare organizations are not built in a way they can identify illegal records; hence, they are unable to eliminate them. 
 Have you ever sought medical care from multiple providers for the same condition? Then you probably already know how difficult it can be to coordinate care from one practice or facility to the next. One provider may not necessarily have access to the test results ordered by another provider, and even getting a prescription filled can be a hassle — you have to wait while the pharmacist fills your prescription and hope that he or she doesn’t misread the prescribing doctor’s terrible handwriting.
Have you ever sought medical care from multiple providers for the same condition? Then you probably already know how difficult it can be to coordinate care from one practice or facility to the next. One provider may not necessarily have access to the test results ordered by another provider, and even getting a prescription filled can be a hassle — you have to wait while the pharmacist fills your prescription and hope that he or she doesn’t misread the prescribing doctor’s terrible handwriting.