By Michelle Barlow, RN, BSN, Director of Product Management Home Health, Homecare Homebase.
Home-based care clinicians are under growing strain, with recent reports showing that 40% of nurses intend to leave the workforce by 2029. Time lost on redundant administrative tasks only adds to this strain.
Care providers spend significant bandwidth on ineffective documentation, with 79% reporting time lost to unproductive charting, time that could otherwise be spent with patients.
In home-based care, time spent on inefficient administrative work can lead to reduced visits, delayed appointments, and fewer patients reached. As agencies work to relieve that burden, many are looking for practical ways to return time to clinicians without disrupting care delivery
Emerging software designed for healthcare, such as AI-driven clinical documentation platforms, can offer a path forward. Still, providers in highly regulated settings remain cautious about adopting tools that interact with sensitive patient information. In home-based care, adoption will depend not just on what AI can do, but on whether it is implemented with the right safeguards. Home-based care agencies should therefore implement AI that prioritizes compliance and clinician judgment, while reducing documentation burden.
Reimagining Documentation to Restore Time for Care
In home-based care, workforce shortages are a contributor to access to care limitations. Since documentation can play a significant role in clinician burnout, integrating AI documentation tools into an agency’s current software stack may help providers prioritize care and open up more capacity to help new patients. Doing so may help avoid an infrastructure overhaul that would further disrupt care delivery.
When effectively layered, these systems can save up to 30%-50% of a nurse’s bedside documentation time by generating draft language or structured suggestions for the Outcome and Assessment Information Set (OASIS) responses based on contemporaneous clinical inputs. AI can also play a constructive role in the revenue cycle, identifying missing claim information and automating eligibility, freeing more time for hands-on patient care.
Yet, there are certain concerns around whether AI will draft documentation for clinician review or independently determine a response. The former approach, where the clinician remains responsible for evaluating, editing, and confirming the final record, is what is needed in today’s healthcare environment to maintain high-quality, individualized care as well as regulatory compliance. Without this emphasis on accountability, automation will lack effectiveness.
Balancing Automation with Accountability
Given patient privacy concerns and stringent HIPAA regulations in decentralized environments, many agencies hesitate to adopt AI that interacts with clinical record systems. Organizations may delay pilots or even pause the adoption of low-risk tools altogether due to regulatory concerns, which can stall the use of workflow-support tools that could ease documentation burden. To address these concerns, agencies should implement solutions that focus on compliance. These approaches should include deliberate safeguards that promote transparency and preserve clinician oversight.
AI in home-based care must support clinician-led, human-in-the-loop processes to maintain compliance. This often looks like care providers monitoring AI-generated summaries and outputs to determine whether they are consistent with source data, suppress unsupported inferences, and avoid hallucinations not grounded in clinical records. Providers are expected to evaluate the suggested documentation content, make any necessary modifications, and confirm the final response.
These systems should also be based on interoperable, clinically meaningful data points. In home-based care, timely visibility into events such as hospital admissions, discharges, and other material changes in patient status. Without that access, AI may be limited in its ability to support preventive intervention or care coordination. At the same time, agencies need to ensure patient data is handled in ways that protect privacy and support compliance, while reducing biased recommendations and security breaches. When these conditions are met, organizations can help improve output accuracy, strengthen audit defensibility, and maintain consistency across records, all without compromising clinician judgment.
Putting Clinicians First in the Age of AI
In home-based settings, patients are medically fragile and reliant on coordinated assistance. Even slight disruptions in timing or service could trigger avoidable hospitalization. Home-based agencies cannot afford the effects of staffing shortages caused by the nurse burnout epidemic. To elevate patient care, home-based organizations should prioritize integrating solutions that ease administrative burden where appropriate and return time to the clinicians delivering care.
Integrating these intelligent systems is not about replacing clinical judgment, but about supporting agencies with tools that reduce unnecessary documentation burden and help reduce burnout. By implementing human-in-the-loop practices alongside AI outputs, home-based agencies can better prioritize provider well-being and, in turn, help patients receive the care they need.
Revenue risk no longer begins and ends with managing denials. It now touches every stage of the revenue cycle — from documentation, charge capture, and coding to billing and denials management — and healthcare organizations relying on reactive, manual, and siloed oversight approaches are paying the price. In an environment defined by financial pressure, heightened regulatory scrutiny, and increasingly AI-powered payer behavior, reactive approaches are no longer enough.
Today, MDaudit, an award-winning, AI-powered continuous risk-monitoring platform. launches “Revenue Integrity Redefined,” a campaign that charts a clear path forward for revenue cycle leaders navigating today’s financial uncertainty. The campaign launches with a flagship video and a suite of supporting resources, including an assessment tool that helps organizations benchmark their revenue integrity maturity across denial prevention, audit readiness, cross-functional alignment, and technology enablement.
Why It Matters: The Stakes Have Never Been Higher
The financial pressures facing healthcare providers are not abstract — they are measurable, accelerating, and compounding. MDaudit’s 2025 annual Benchmark Report documents the scale of the challenge:
Coding-related denials increased by as much as 26%
Medicare Advantage average denied amounts rose 20%
Medical necessity and RFI denial amounts increased by 70%
Payer audit volume and dollars at risk rose 30%
Initial response times for claims take more than a month across all claim types
These trends reach far beyond the revenue cycle team. They affect operating margins, forecasting accuracy, workforce planning, and capital investment decisions — making revenue integrity a C-suite and board-level concern.
Ritesh Ramesh
“Denials are rising, payer audits are expanding, and reimbursement timelines are longer than ever,” said Ritesh Ramesh, Chief Executive Officer of MDaudit. “The weight these realities place on everyone who touches the revenue cycle is enormous. The path forward is integrity in compliance documentation, coding, and billing practices, enabled by real-time data and AI-powered technologies, and trusted partnerships chosen to support revenue cycle teams.”
Compounding these pressures is an accelerating AI arms race between payers and providers. Payers are automating denials faster than ever, while providers scramble to keep pace.
Health system CFOs across the country are confronting the same paradox: AI is simultaneously the problem and the solution with the highest potential. How quickly organizations can move past theoretical conversations and execute actions to deliver ROI with AI may define their financial health for years to come.
MDaudit’s Answer: Meaningful, Not Artificial, AI
MDaudit was built for this moment. Rather than layering AI on as an afterthought, MDaudit embeds intelligence as a horizontal layer woven throughout the platform. The result is the Meaningful AI framework — a deliberate, outcomes-driven approach designed to deliver measurable ROI, not automation for its own sake.
MDaudit’s AI-powered solutions below delivered more than $500 million in ROI across its customer base in 2025. These solutions have done the heavy analytical lifting and leveraging of automation, while keeping humans in the loop.
These solutions include:
Payer Audit Workflow automatically extracts and organizes information needed from Additional Documentation Requests (ADRs) with SmartScan.ai, which compresses a process that once took days into minutes — accelerating provider response times and reducing administrative strain. Customers retained over 375 million in total revenues in 2025 by responding to payers in a timely and efficient manner
eValuator applies AI-powered rules to interrogate pre-bill charges across facilities, specialties, and multiple EHR and billing systems — surfacing encounters that require correction before a claim is ever submitted. The result: net revenue capture, stronger compliance posture, and costly denials prevented before they start. Customers have driven a total financial impact of more than 140 million in 2025 by taking a proactive approach with eValuator to ensure coding integrity
AI Assist democratizes access to strategic insights across the entire organization. Users at every level — including the C-suite — can ask questions in plain English and receive answers instantly, without reliance on report writers or technical interpreters. Data-driven decision-making becomes accessible to everyone who needs it.
“The most important questions for health systems implementing AI are: Is this technology reliable, secure, and meaningful to drive ROI? MDaudit has taken a first principles approach to these questions while developing our solutions,” said Ramesh.
Revenue Integrity Redefined: From Reactive to Confident Control
Modern revenue integrity unites revenue growth and risk mitigation into a single, connected framework. With real-time data, AI, and automated workflows, leaders gain early visibility into risk, clearer performance insights, and the ability to intervene before issues escalate into financial loss or regulatory exposure.
The strongest outcomes emerge when silos between compliance, coding, revenue cycle, and clinical teams are broken down, and when objective data drives prioritization, accountability, and cross-functional alignment.
MDaudit case studies across multiple health systems consistently demonstrate what that looks like in practice: expanded audit coverage without proportional staffing increases, measurable improvements in coding accuracy, significant reductions in denials, early identification of multimillion-dollar risk exposure, and increased executive visibility through defensible benchmarking.
This is revenue integrity redefined.
“Organizations that treat revenue integrity as a mission-critical capability supported by continuous monitoring and intelligent automation are better positioned to navigate payer complexity, workforce shortages, and regulatory expansion,” said Ramesh. “By moving from reacting to denials to anticipating risk, from defending audits to preventing them, and from fragmented oversight to confident control, MDaudit empowers revenue cycle teams to achieve outcomes that matter.”
Availity, the nation’s largest healthcare network connecting payers, providers, and technology partners, today unveiled Availity Extend, a new way to build automation and AI on the Availity network. Availity Extend lets organizations securely empower automated workflows by leveraging Availity’s existing connectivity, payer integrations, and trusted security framework, coordinating execution with live network data and logic, rather than relying on copied or externalized data.
With AI and automation already widely deployed across healthcare operations, the real constraint is not intelligence, but whether those systems can execute across governed, real?world workflows. Fragmentation—critical information and decision logic spread across organizations and systems that must remain tightly aligned—continues to limit scale, speed, and reliability. Automation only works at scale when it operates with full context and within trusted frameworks.
With Availity Extend, automation operates within existing identity, security, and compliance frameworks, with full auditability by design.
“AI in healthcare can’t stay confined to individual systems—it needs to operate across the workflows that directly connect payers, providers, and partners,” said Russ Thomas, Chief Executive Officer of Availity. “Availity Extend is designed to make that possible in a way that reflects how healthcare actually works: across organizations, within trusted frameworks, and at national scale.”
Making the Network Buildable
For more than 25 years, Availity has provided the neutral trust layer connecting payers and providers across core operational workflows, powering more than half of all U.S. healthcare activity each year. Today, the Availity network directly connects more than 4,000 payers and 3.5 million providers, with direct connectivity into payer systems, providing deeper access to payer logic, earlier in the workflow, where decisions can be made more accurately and efficiently.
Availity Extend builds on that foundation by providing a governed, network-connected way to develop and orchestrate automation across the Availity network. Through a standardized activation layer, payers and technology partners can coordinate end?to?end automation and agent?driven workflows in alignment with existing network logic, connectivity, and controls.
“Organizations across healthcare are investing heavily in automation and AI,” said Sean Barrett, Chief Product Officer of Availity. “Availity Extend allows those investments to focus on real operational outcomes—without recreating foundational connectivity or governance.”
What Differentiates Availity Extend
Coordinated workflows, not point?to?point APIs. Availity Extend enables end?to?end execution that maintains context across payer and provider workflows—producing completed outcomes rather than disconnected data exchanges.
Live network context, not replicated data. Because Availity Extend coordinates with live network data and logic, workflows stay aligned with real?time requirements and controls already enforced across the Availity network. Organizations can coordinate eligibility, authorization, clinical data, claims, and payment steps within a single automated workflow—without expanding access or introducing new data permissions.
Intelligence that compounds over time. Organizations that build on Availity Extend benefit from network?level insights that accumulate with use—informing automated and AI?driven workflows across real healthcare interactions.
Security and governance by design. All automation runs within Availity’s existing security, identity, and governance framework—the same framework that governs more than half of U.S. healthcare administrative transactions each year.
Looking Ahead
Availity Extend marks a shift from connecting healthcare systems to enabling real action by making the Availity network buildable, allowing automation and AI, including agent?driven workflows, to move from isolated use cases to coordinated, system?level execution, where governance, context and trust are enforced by design. Availity Extend is how that future becomes real.
Availity Extend is being rolled out with an initial set of content and customers in the first half of 2026, with broader availability planned later in the year.
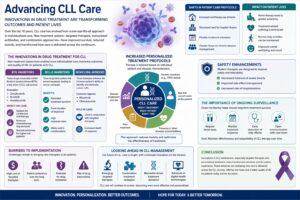
Over the last 10 years, Chronic Lymphocytic Leukemia care has moved from a one-size-fits-all approach to more individualized care because of the multitude of treatment options that have become available Most Chronic Lymphocytic Leukemia therapies involve the use of traditional chemotherapeutic agents, which are known to have a high toxicity as well as a high rate of hospital re-admissions.
Otherwise, the treatment may involve immunotherapy, immuno-chemotherapy, or even combinations of these approaches. The clinical evidence suggests, however, is that these therapies have not only been shown to enhance patient survival, but more importantly, they have begun to alter the way care is delivered throughout the continuum of Chronic Lymphocytic Leukemia management.
The Innovations in Drug Treatment for CLL
The last decade has seen multiple developments in treatment options for Chronic Lymphocytic Leukemia. Chronic lymphocytic leukemia medication has been transformed by the Introduction of Targeted Therapies, as they have centered the focus of care on the patients be treated and the care that is provided.
Targeted therapies have been instrumental in establishing patient-centered care by enabling the development of new and innovative Treatment classes that, for example, improve the continuity of care by lowering the amount of time patients spend in the hospital and by offering more options in the management of their disease, which, in turn, supports their survival. Moreover, care providers are interacting with patients more frequently, which, in addition to addressing the patients’ needs, helps to improve their treatment outcomes.
The Introduction of New Treatment Options in CLL Management
The development of Targeted Therapies has provided more individualized options, resulting in the inception of new Treatment classes with markedly improved side-effect profile, which have been integrated into the lexicon of the treatment of patients with Chronic Lymphocytic Leukemia. An example of this would be the use of drugs that are classified as irreversible Bruton’s tyrosine kinase inhibitors, which selectively inhibit the activity of Bruton’s tyrosine kinase.
The following examples pertain to Bruton’s tyrosine kinase (BTK) inhibitors:
Zanubrutinib
Ibrutinib
Acalabrutinib
Impact on Care:
Options for continuous oral therapy
Reduced chemotherapy requirements
Studied outcomes for higher risk patients
BCL-2 Inhibitors
These drugs cause the death of cancer cells because of the inhibition of proteins that block the process of apoptosis.
Benefits:
Extended treatment duration
Fixed duration of treatment
High response rates
Works well in combinations.
Monoclonal Antibodies
These therapies improve the immune system’s ability to identify and eliminate cancer cells.
Common Agents:
Rituximab
Obinutuzumab
Role in Care:
Used in conjunction with targeted therapies
Increased depth of response
Increased Personalized Treatment Protocols
A key influence of the current chronic lymphocytic leukemia medication is the focus on personalized medicine. Therapeutic options are determined by the patient’s genetic profile, the disease’s progression, and other individual characteristics.
Some of the factors include:
Genetic mutations (e.g. TP53 status)
Age and overall health of the patient
Presence of other diseases (comorbid)
Prior treatment
This approach to care reduces toxicity to the patient and optimizes the effectiveness of the treatment.
Shifts in Patient Care Protocols
Advancements in medication have also restructured how care is delivered.
The following changes have occurred:
Increased oral therapy use at home
Decreased need for hospital infusion
Flexible treatment schedules
Greater focus on chronic disease management
These changes have improved access to and ease of care for patients.
The goal of modern therapy is to improve safety and tolerability while still minimizing side effects. This is particularly important for the elderly, who form a large part of the population with Chronic Lymphocytic Leukemia.
Safety Enhancements:
Decreased instances of severe toxicity.
Improved side effect management.
Decreased rate of hospitalizations.
This has allowed for the uninterrupted continuity of treatment for even more patients.
Importance of Ongoing Surveillance
With the advent of targeted treatments, often, oral, ongoing surveillance has integrated into treatment guidelines.
Surveillance Techniques:
Blood drawings at intervals are essential.
Treatment response timelines must be adhered to.
Side effects must be monitored at the earliest possible junctures.
Communication to medical authorities must be unrestricted for the full duration of the study.
Goals of surveillance include ensuring that CLL therapeutics remain effective for as long as possible.
Influence on the Life of the Patient
Improved quality of life for patients is the greatest benefit derived from all advances in the treatment of Chronic Lymphocytic Leukemia.
Benefits:
Home therapy leads to a greater degree of autonomy.
Treatment related suffering is diminished.
Normal functions of daily life can be performed.
Mood is elevated.
Some patients can maintain daily activities while undergoing treatment, depending on individual response and disease characteristics.
Barriers to New Protocols Implementation
Despite the progress in the field of Chronic Lymphocytic Leukemia therapy, barriers remain to the application of newly developed approaches to standard practice.
Main Barriers:
Targeted therapies are expensive.
Patients must be willing to buy into the treatment for the duration of its implementation.
There is the possibility of developing resistance to the pharmacologic agents that may be used.
Pharmacologic agents that are used may interact adversely.
The remaining barriers must be addressed to optimize the new approaches to treating Chronic Lymphocytic Leukemia.
Looking Ahead in CLL Management
Innovations in targeted therapy remain the focus in the management of Chronic Lymphocytic Leukemia. It is anticipated that Chronic Lymphocytic Leukemia therapy will still be improved in the near future, providing an even greater degree of personalization.
What to Expect:
Targeted therapy that is emerging.
Strategies that include more than one treatment.
Treatment choices based on specific biological markers.
New technologies that include digital health.
The treatment of Chronic Lymphocytic Leukemia will be even more effective than it is now.
Conclusion
Recent progressions in chronic lymphocytic leukemia medications have been invaluable in providing quality management strategies for this disease. The innovations with respect to Chronic Lymphocytic Leukemia medications include targeted therapies and personalization of treatment plans. These developments have influenced how care is delivered across different stages of Chronic Lymphocytic Leukemia management. Modern medications for Chronic Lymphocytic Leukemia have also helped in simplifying the process for care givers and have also drastically improved the Chronic Lymphocytic Leukemia patient experience. The ongoing research in this field of study will ensure that the Chronic Lymphocytic Leukemia management will be at the apex, and ensure that the patients will have hope, and live better, in the future.
Every few months, another health system announces it has deployed artificial intelligence across its revenue cycle. The press release follows a familiar script: reduced denials, fastero authorizations, staff hours reclaimed, efficiency unlocked. What almost never appears in that announcement is a second document, the one that defines how the organization will know, 12 months from now, whether any of that is actually true.
That absence is not an accident. It reflects something deeper about how healthcare has historically treated its administrative infrastructure: as a problem to manage rather than a system to understand. And now, as AI tools move from pilot programs into operational deployment at scale, that gap is now creating real operational risk as AI moves into live production environments.
I have spent more than twelve years working alongside revenue cycle teams, coders, billers, authorization specialists, and CFOs, and I can say with some confidence that most of the people closest to this work are deeply skeptical of headlines. They have seen technology promises before. They remember the EHR implementations that were supposed to streamline documentation and instead added hours to the physician workday. They remember the clearinghouse upgrades that reduced one bottleneck and created three others downstream. They are not cynics. They are people who have learned, through experience, that what a system claims to do and what it actually does inside a live operational environment are often very different things.
That skepticism is not resistance to change. It is exactly the kind of operational discipline that should shape how AI gets evaluated and deployed.
The challenge right now is that the industry has skipped that step. Conference stages are crowded with transformation narratives. Health systems facing tight margins and persistent staffing shortages feel genuine urgency to find operational relief. All of that is understandable. But urgency without accountability is how you end up automating broken processes rather than fixing them. And in the revenue cycle, broken processes do not just affect the balance sheet. They affect whether a patient gets a procedure approved on time. They affect whether a physician burns another hour on paperwork that should have taken ten minutes. They affect the trust that providers, payers, and patients depend on to make the system function.
What I find missing in most AI deployment conversations is a straightforward commitment to answering a basic question before the contract is signed: what does success look like, and how will we measure it independently? Through clean, pre-specified performance benchmarks, first-pass resolution rates, authorization turnaround times, denial overturn rates, measured against a documented baseline and evaluated at regular intervals by people inside the organization who are empowered to say when something is not working.
Part of the reason is structural. Revenue cycle operations in most health systems sit in a complicated organizational space, accountable to finance, connected to clinical operations, dependent on technology infrastructure managed by IT, and constrained by payer relationships that nobody controls entirely. That diffusion of accountability makes it genuinely difficult to assign ownership over AI performance. When a denial rate creeps up six months after an AI tool goes live, the question of who is responsible for diagnosing why, whether the technology team, the RCM leadership, or the vendor, rarely has a clean answer. So the question often goes unasked, or gets absorbed into the background noise of operational management.
The other part is cultural. Healthcare administration has a long tradition of accepting complexity as inherent rather than examining it as designed. Prior authorization, to take the most visible example, has become so procedurally dense that many organizations have simply built workforces around navigating it rather than questioning whether the navigation itself can be fundamentally restructured.
The scale of that problem is not abstract: according to CMS, more than 53 million prior authorization requests were submitted to Medicare Advantage insurers in 2024 alone, and of the denials that were appealed, more than 80% were ultimately overturned. AI can reduce the friction of that navigation. But if the underlying logic of the process remains unchanged, if the criteria are still opaque, the payer responses still inconsistent, the documentation requirements still disconnected from clinical reality, then automation speeds up a broken system without healing it. That is a meaningful difference, and it is one that outcome measurement frameworks need to be designed to capture.
What better practice looks like, in my view, is fairly concrete. It starts with a pre-deployment audit with a clear-eyed inventory of where the revenue cycle is actually failing, not where it looks like it might benefit from technology. It requires that AI tools be evaluated against those specific failure points, with defined thresholds for what improvement looks like at thirty, ninety, and one hundred eighty days.
It demands that operational staff, the people who work inside these processes daily, have a formal mechanism to surface when a tool is creating new problems, not just solving old ones. And it insists that model performance be reviewed on a scheduled basis, because the payer landscape does not hold still, and a model trained on last year’s coverage criteria may be quietly degrading against this year’s.
None of this is technologically complicated. It is organizationally disciplined. And that distinction matters, because the conversations health systems need to have about AI accountability are not primarily conversations with vendors. They are internal conversations about how seriously the organization intends to govern its own operations.
Policymakers have a parallel responsibility. As federal and state attention increasingly focuses on prior authorization reform and payer transparency, there is an opportunity to embed outcome reporting requirements into any regulatory framework that governs automated administrative decision-making. An AI system that accelerates a payer’s denial process without improving clinical appropriateness is not a healthcare innovation. It is an efficiency tool for the payer, not an improvement in care decision-making. Regulators should require that distinction to be measurable and reported, not left to vendor interpretation.
The potential here is real. The revenue cycle absorbs an extraordinary share of healthcare resources, resources that could otherwise support direct patient care, workforce retention, or capital investment in underserved communities. Thoughtful AI deployment, governed by rigorous measurement, can free up meaningful capacity across the system. I have seen it work in contained, well-designed implementations. The problem is not that the technology cannot deliver. The problem is that without accountability frameworks, we will not actually know when it does, and we will not catch it when it does not.
Healthcare has spent years debating what AI can do. It is past time to build the infrastructure to find out what it is doing.
By Jaylee Hilliard, MSN, RN, NEA-BC, CPXP, Vice President of Clinical Strategy, AngelEye Health.
In many neonatal intensive care units (NICUs), bedside cameras are still treated like an optional amenity. That framing no longer aligns with the reality of modern neonatal care or with what families experience during prolonged separation.
In one study, only 22% of parents with bedside camera access described separation from their infant as extremely stressful, compared to 63% of parents without access. The question is no longer whether families value virtual visibility, but why access remains inconsistent across units and health systems.
For many families, separation from their child is an unavoidable part of the NICU experience—not from lack of desire, but because medical acuity, postpartum recovery, distance, work, and caregiving responsibilities make around-the-clock presence nearly impossible. Even in units with open visitation, most units are not structured with private rooms or accommodations that allow families to remain at the bedside overnight. Parents must balance learning their infant’s care plan, participating in bedside rounds, and preparing for discharge during the limited hours they can be there.
When access to the bedside becomes inconsistent, stress rises. The NICU experience is emotionally intense for many families, and prolonged separation often intensifies that strain. Beyond physical distance, uncertainty between clinical updates or overnight when parents cannot be present can compound anxiety and make an already difficult experience feel overwhelming.
Visual access is not a substitute for bedside participation, but it can reduce uncertainty during unavoidable separation. When hospitals treat bedside cameras as essential infrastructure, they acknowledge how NICU stress truly manifests and can address it with tools that protect privacy, support clinicians, and integrate seamlessly into care delivery.
Visual Access as a Component of Family Integrated Care Family integrated care has long shown that meaningful parent participation in care and decision-making supports better outcomes for both infants and parents. Bedside cameras do not replace hands-on caregiving, skin-to-skin time, or bedside teaching. Rather, they serve a complementary function: maintaining connection when physical presence is not possible.
Studies have linked real-time video access to improved parental well-being, a stronger sense of involvement, and greater trust in the care team. That connection matters clinically as distress can affect how families process information, stay engaged over long hospitalizations, and build confidence for discharge.
The question, then, is not whether cameras offer value, but whether they’re implemented well and equitably.
Operational Integration: Designing Cameras That Support Families and Care Teams
When bedside cameras are deployed with clear privacy standards and defined workflows, they stop functioning as isolated tools and begin operating within the care model itself. In practice, families use visual access during the hours they cannot be physically present and when bedside participation isn’t feasible. Overnight, during recovery, or while balancing work and other responsibilities, cameras extend connection beyond hospital walls in a structured way when other real-world constraints prevent physical presence.
For care teams, the difference is operational. Despite concerns of adding another technology to manage or another tool to navigate, when implemented with clear governance, cameras can support continuity without adding burden. Cameras Support communication consistency across shifts, reduce information gaps between updates, and align with broader efforts to make family-integrated care reliable rather than dependent on individual practice styles. The real distinction is not whether a unit simply has cameras, but whether that visual access is intentionally designed into the clinical environment.
Without defined expectations, visual access can feel informal and unpredictable. With governance structures such as one-way video, pausing during hands-on care, and consistent communication norms, expectations become standardized. Families understand what they will see, when it may pause, and how to escalate questions appropriately. This clarifies boundaries for both clinical staff and parents.
What Standardized, Scalable NICU Camera Programs Get Right
Inconsistent enrollment and informal workflows can unintentionally create access gaps. When visual access depends solely on staff reminders, language availability, or passive opt-in processes, some families receive full support while others are left navigating the system on their own. Standardization prevents that variability. A standard-of-care approach is not “install cameras and hope for the best;” it’s a deliberately designed, burden-light program with clear operating norms:
One-way team-to-family micro-updates (photo/video/text) that are brief, consistent, and easy to standardize across shifts.
Proactive enrollment at admission, integrated with existing workflows (not passive opt-in) and supported by plain-language, translated instructions.
Privacy-protective operations by default, including pausing during hands-on care and no audio.
Language access built into the platform rather than added later.
Ongoing monitoring of activation and use by language, insurance, and distance, with targeted support when gaps appear.
Designing and operationalizing NICU camera programs is practical and cross-functional, requiring coordination among clinical leadership, patient experience, IT/security, and NICU operations to support safety, trust, communication, workforce experience, and equity.
Moving the Frame From “Amenity” to Expected Care
NICUs standardize practices to reduce harm and improve outcomes. NICUs standardize practices to reduce harm and improve outcomes. Over time, interventions such as standardized handoffs, barcode-based safety checks, and structured discharge-readiness workflows have shifted from “nice to have” to expected care. Bedside cameras—implemented with privacy safeguards and equitable access—fit that same evolution.
Bedside cameras, when implemented with strong privacy safeguards and equitable access, align with that same purpose. They support connection during unavoidable separation, reinforce trust, reduce unnecessary communication strain, and help extend family participation beyond visiting hours.
Treating visual access as a dependable component of care, rather than a discretionary add-on, requires planning and governance, not improvisation. Clear expectations for families, consistent staff workflows, privacy-first controls, and active monitoring for equitable access are what distinguish a technology feature from care infrastructure.
In NICU care, “must-have” capabilities are those that standardize safety and reduce variation over time and across staff. With privacy-first governance and workflow integration, bedside cameras meet that bar—shifting from an optional feature to dependable infrastructure.
The real question is not whether cameras feel family-centered, but whether they function like other NICU-critical systems: standardized, governed, equitable, and reliable across every shift.
Relationships between healthcare organizations and insurers play an important role in providing proficient care. Yet, administrative circumstances, often beyond a medical group’s control, strain payer-provider relations.
Operational structures often leave healthcare personnel navigating disconnected communication channels, inconsistent formats, and slow reimbursement timelines, creating friction between medical teams and those providing payment for their services. The Healthcare Financial Management Association (HFMA) reports that nearly 87% of provider CFOs believe strained payer relationships impact their ability to provide optimal care.
Staff also feel the toll of redundant reconciliation work, which contributes to burnout and frustration with clunky administrative systems. An occupational health survey by the Public Health Reviews journal found that 70% of respondents reported burnout symptoms, with dissatisfaction tied to administrative processes among the factors. These burdens aggravate staff wellbeing and the tense interactions between medical systems and payers.
To lessen administrative exhaustion and the breakdown of trust between the industry and carriers we work with, systems and practices alike will benefit from understanding the financial pain points and how adopting modern payment strategies can reduce monetary burdens.
The Disconnect: Banks and Providers
Banks and other financial institutions are not HIPAA-covered entities, meaning they are limited in how they handle patient-specific remittance data, further fueling the disconnect between payers and providers. This limitation, further worsened by legacy methods such as paper checks, ACH transfers, and standalone 835 files, causes healthcare professionals to juggle between parallel systems to transfer necessary information to the proper recipient, resulting in additional costs and errors.
Reconciling installments using these labor-intensive approaches can contribute to higher claim denial rates. The American Hospital Association found that private payers denied nearly 15% of all claims at initial submission. With rising healthcare costs pressuring affordability, patients often struggle with delays caused by inconsistent claim resolutions. When claims go unresolved, trust between medical groups and insurance providers becomes significantly more important to positive patient outcomes.
Simplifying how claims are returned and processed helps with these delays. Accelerated claim adjudication offers a practical path to help rebuild trust in the reimbursement process. To accomplish this task, our sector must empower banks with the necessary information to address repayment concerns quickly.
Cutting Administrative Drag in Reimbursement
Healthcare facilities can reduce manual work by embedding HIPAA-compliant data directly into each financial transaction. When payment and remittance data travel together, staff spend less time re-associating settlements with separate 835 files after processing, reducing errors associated with fragmented formats.
Any modernization effort must also protect sensitive information. Accomplishing this requires building encrypted, PCI- and HIPAA-compliant data paths that safeguard patient privacy. By unifying financial and clinical information into a single system, with secure guardrails, providers eliminate the need for multiple platforms.
Modern payment software supports this approach by unifying reimbursement and remittance into a single, automated flow. These platforms can securely post payments in real time to practice management systems (PMS), electronic medical records (EMR), and electronic health records (EHR).
Practices that integrate automated payer reimbursement platforms into their existing systems can standardize explanation of payments (EOP), permitting the replacement of inconsistent layouts. This digitization enables one-click posting, supporting accuracy and reinforcing audit readiness for large and small healthcare organizations.
Including encrypted data in payment transactions reduces errors and administrative redundancies across all stages of the reimbursement cycle, helping fuel smoother fiscal experiences between coverage organizations and providers.
A Smoother Path From Claim to Payment
Reducing errors helps ensure minimal denials and faster claim turnaround times. This diminishes accounts receivable, cuts reimbursement processing time, and improves cash flow. Practices that minimize payment inefficiencies free practitioners to focus on patient-facing care, reducing burnout tied to administrative systems, and restoring attention to critical healthcare priorities.
With minimal payment inefficiencies, the disconnect between insurers and medical groups will lessen, further strengthening payer-provider relationships. This will, in turn, allow care recipients to divert their attention from the burden of denied financial claims to what’s most important: recovery.
As healthcare finance keeps shifting, organizations that implement strategies to strengthen financial relationships will be better suited to help payers, providers, and patients thrive.
Marchex, which harnesses the power of AI and conversation intelligence to provide actionable insights derived from prescriptive vertical-market data analytics, today announced the launch of a new integration with Freshpaint, a platform built for healthcare marketers to deliver measurable performance while safeguarding patient trust in a complex regulatory environment.
Freshpaint’s data platform enables healthcare organizations to securely connect and activate data across channels, so that they can link marketing spend to outcomes while safeguarding patient privacy and complying with industry regulations.
Empowering Healthcare Marketers with Stronger Outcomes
The Marchex-Freshpaint integration allows healthcare marketers to seamlessly connect rich inbound call and conversation data with downstream marketing platforms, so that they can easily associate digital marketing activity with phone-based patient scheduling, without putting protected health information at risk. By leveraging advanced data capture and attribution, healthcare organizations can drive stronger marketing outcomes while operating compliantly within highly regulated healthcare environments, unlocking new opportunities for campaign optimization, patient segmentation, and patient journey management.
“Integrating Marchex’s industry-specific conversation intelligence with Freshpaint’s leading privacy-by-design infrastructure gives marketers clearer visibility into the patient interactions that shape demand,” said Troy Hartless, President and CRO at Marchex. “Together, we’re enabling organizations to activate conversation data with precision, tie marketing efforts directly to booked appointments, and unlock more efficient growth across the patient journey.”
“Healthcare marketers are under pressure to drive measurable growth on fixed budgets, and they shouldn’t have to choose between performance and compliance,” said Ray Mina, CEO at Freshpaint. “By combining Marchex’s conversation intelligence with Freshpaint’s privacy-first infrastructure, we’re helping teams turn privacy into a strategic advantage — so they can connect data to real appointment outcomes, prove what works, and optimize campaigns with confidence.”
Through Marchex’s AI-powered conversation intelligence solution, integrated with Freshpaint, healthcare marketers gain deeper insights into patient access, appointment scheduling outcomes, and patients’ call-driven care navigation as they manage their care.
Driving Innovation and Differentiation
Uniting Marchex’s conversation intelligence with Freshpaint’s compliant data infrastructure, healthcare marketers can elevate appointment volumes and patient acquisition through campaign optimization and improved automated bidding that attract more targeted, high-value leads.
Integration Features and Benefits
Advanced Data Capture – Marchex captures and securely transmits call events to Freshpaint, including session data, attribution details, and rich conversation signal data, such as sentiment, patient type, lead outcome, and topics, fueling better patient acquisition outcomes through more precise targeting, attribution, and journey insights.
Comprehensive Marketing Capabilities – The integrated solution enables clients to optimize campaigns, segment audiences, track patient journeys, and attribute marketing performance to scheduled appointments or visits, while complying with healthcare privacy regulations.
Patient Journey Completeness – The integration supports both session-based and offline calls, giving teams more comprehensive insights into the patient journey and the touchpoints that drive appointments and visits.

 Over the last 10 years, Chronic Lymphocytic Leukemia care has moved from a one-size-fits-all approach to more individualized care because of the multitude of treatment options that have become available Most Chronic Lymphocytic Leukemia therapies involve the use of traditional chemotherapeutic agents, which are known to have a high toxicity as well as a high rate of hospital re-admissions.
Over the last 10 years, Chronic Lymphocytic Leukemia care has moved from a one-size-fits-all approach to more individualized care because of the multitude of treatment options that have become available Most Chronic Lymphocytic Leukemia therapies involve the use of traditional chemotherapeutic agents, which are known to have a high toxicity as well as a high rate of hospital re-admissions.


