Guest post by Abhinav Shashank, CEO & Co-founder, Innovaccer.
Abhinav Shashank
Whatever we do in the healthcare space, it is eventually meant for the greater good of patients, which is why today the aim of modern healthcare is shifting towards value-based reimbursement and with that the process is getting modified accordingly. Gradually, patient-centric care is becoming prevalent. The current standards require enhanced patient experience, and that comes with improved quality, coordinated care at a reduced cost.
CMS when releasing the fact sheet for Hospital Value-Based Purchasing Program for the year 2016, said in a statement, “We now pay hospitals for inpatient acute care services based on the quality of care, not just the quantity of services provided.” Backing this statement was the fact that out of the four quality domains, patient experience of care bore 25 percent of the weight. This led to hospitals working earnestly towards enhancing the patient experience and utilizing the massive potential to qualify for the bonus and improve on current standards.
Why does Patient Experience Matter?
Patient experience is an essential component of the IHI Triple Aim, a schema for elevating the standards of providers’ performance:
Improving the patient experience of care.
Improving population health.
Reducing the per capita cost of healthcare.
Fortunately, health systems know that patient satisfaction isn’t just a tool for a performance bonus. Improving patient satisfaction is a way to identify gaps in care delivery and develop quality services. Also, according to a survey conducted by a health system found that out of 1,019 adults interviewed, 85 percent were dissatisfied with at least one aspect of their providers. Creating a patient-centric industry where experience and satisfaction of patients are overlooked is almost impossible!
Improving Patient Experience
A lot of researches have established that improving patient experience directly results in higher quality of care. Healthcare systems have realized the importance of the Triple Aim, and here’s how they can start working in this order on improving one of the fundamental aspects:
Patient Engagement a Priority
Patient engagement has been one of the most talked-about aspects of healthcare and unquestionably a way to improve the care experience. What we need to ensure is that the patient is willing to participate in the decision-making and the provider advocating this intervention. Even though healthcare providers are making efforts to improve patient engagement at their end, a survey revealed that only 34 percent of the patients are highly encouraged. Some effective methods patients found useful are:
59 percent of the surveyed people found increased physician-patient time vital.
54 percent of the patients favored being part of the decision-making.
36 percent promoted the growth of patient access to services.
Using Data Analytics
Data analytics have proven their worth in healthcare, and we have only scratched the surface of the immense sea of possibilities that can be realized using data analytics. When it comes to advancing patient experience, data analytics can be used in several ways:
Gathering data and creating actionable follow-up plans for patients.
Leveraging data analytics for accurate analysis of patients and reducing readmission rate.
Data analysis can zero in on inefficiencies and medical errors and help reduce avoidable expenses.
In the current era, it is important to understand the role technology plays in different industrial sectors. The different verticals of the medical industry have adopted technology and identified the benefits associated to it. Healthcare and other medical services can be easily accessed with the help of a smart phone. It has become more convenient to track, regulate, and monitor several medical cycles such as medicine intake, therapy, and treatment. The communication gap between the patients and doctors has reduced over the years owing to advancements in technology. Progressive Markets recently added a market report that offers useful insights related to the global telemedicine market such as market share, size, and growth. The digitalization in medical field is set to facilitate enhanced healthcare and medical services in the coming years.
Technology has revolutionized several industries worldwide over the last two decades. The onset of innovative and modern technological advancements have made a notable difference in the medical field and has made telemedicine a game-changing way to serve people throughout the world. The adoption of telemedicine has increased significantly in the last decade although there are a few concerns regarding its reliability and precision. Approximately more than 70 percent urgent illness conditions can be taken care of with the help of telemedicine according to the American Telemedicine Association. A simple physician training enables providers to diagnose and treat minor problems such as pharyngitis, sinusitis and upper respiratory illnesses with the help of video chat.
General awareness related to telemedicine technology is growing
Telemedicine technology has not flourished largely yet as it is still in the nascent stage. However, as awareness related to the telemedicine is growing, the adoption rates are set to grow. The benefits associated to telemedicine are gradually making a mark in the medical industry. Telemedicine has largely helped to save time. With the help of telemedicine, a patient does not have to travel to the provider and save time.
Further, telemedicine eliminates any chances of transmitting infectious diseases from a patient to the health care professional. Telemedicine saves time and offers time-efficient solutions. However, there are additional benefits associated to it. It reduces costs significantly. The most important aspect of telemedicine is its ability to cater to the needs of the patients from any place at any given time. This is highly beneficial for occupational medicine. Telemedicine helps to formulate an efficient and reliable healthcare plan.
Benefits of telemedicine
Telemedicine is making its mark worldwide and it is important to realize that the technological advancement does not eliminate visits to traditional doctors. There are a few medical conditions that cannot be diagnosed without the presence of the patient. However, with data such as medical history of the patient, visual exam and an interview with the patient along with the providers training of pattern recognition, it is convenient to treat patients without them being physically present in the room.
Schumpeter considered it the “essential fact about capitalism,” that things have to fall apart so better things can take their place. The familiar is violently displaced by the unfamiliar, but superior, alternative.
Buggy whip makers are sent out of business as car makers take over the transportation space. Typists go extinct as word processing becomes cheap and ubiquitous. Blockbuster goes bankrupt, so Netflix and all its streaming peers can take over the space. The notion that the New can mean bad news for the Old is nothing unique to our modern era, though perhaps the speed and distribution of change thanks to globalization and digital technology means we see this more and more.
Well, 2017 may well be the beginning of the end for primary care as we once knew it.
The “Who’s on First” of Healthcare
As with any other example of creative destruction, the signs in primary care have been there for anyone to read, though perhaps the conclusion they point to hasn’t been quite as clear as the contributing forces.
Nursing, as a profession, has been on a long arc over the last century or so, transforming patient care as well as clinical organization and even leadership. Nurses have evolved from subordinates to doctors to, in some cases, replacements–notably, in primary care clinics, especially critical access hospitals or in areas where patients might not otherwise get to see a doctor outside of an emergency room.
Primary care provider shortages aren’t strictly limited to rural or remote areas. Thanks to demographic trends, more people are living longer and managing more chronic conditions. Keeping this swell of aging patients from charging into Emergency Departments en masse was part of the logic behind elements of the Affordable Care Act shifting resources to clinics run by NPs as opposed to MDs. While nurses face a shortage of their own, they have still been tagged as a key element of preserving and expanding access to primary care. In 2007, the shift in nursing toward a more central leadership role was codified by the Association of Colleges of Nursing with its designation of the Clinical Nurse Leader as a new official role for nursing professionals.
Simply put, consistent access to primary care supports prevention strategies, which are altogether cheaper and more effective than sending everyone through an ED or into a long-term care clinic. While many–notably, the American Academy of Family Physicians and the American Medical Association–muckrake over this disruption of scope of practice, the change is one of necessity. Nurses today provide critical care, and lead diverse clinical and professional teams to coordinate whole-person health.
With or without the Affordable Care Act, the shortage in primary care will persist. Expanded access through insurance only exacerbated the underlying issue. As Millennials enter middle ages and Boomers carry on retiring and living longer than ever, primary care will be stretched. Whatever comes out of the Trump administration or the ongoing scope of practice debates, primary care requires providers, and nurses are showing up to work.
Guest post Ken Perez, vice president of healthcare policy, Omnicell.
Ken Perez
During the 2016 presidential campaign, Democratic candidate Hillary Clinton reiterated the longstanding Democratic pledge to allow Medicare to negotiate drug prices and demand higher rebates for prescription drugs. In response, and aware of the general public’s mounting concern about rising prescription drug prices, Donald Trump shifted to the left and repeatedly called for Medicare to directly negotiate drug prices. For example, at an MSNBC town hall on Feb. 17, 2016, Trump said, “If we negotiated the price of drugs, Joe, we’d save $300 billion a year.”
However, none of Trump’s three most substantive policy statements issued in the fall of 2016—including the healthcare section of the Trump-Pence Campaign website, his “Contract with the American Voter,” and his healthcare plan issued two days after the election—mentioned the challenge of rising drug prices or the idea of Medicare negotiating drug prices with pharmaceutical companies.
On Jan. 31, 2017, President Trump met with a group of pharmaceutical industry executives, including the CEOs of Amgen, Celgene, Eli Lilly, Johnson & Johnson, Merck, and Novartis, as well as Stephen Ubl, head of the Pharmaceutical Research and Manufacturers of America (PhRMA).
While during the meeting Trump called drug prices “astronomical” and said, “We have to get prices down for a lot of reasons … for Medicare and Medicaid,” he stopped short of the aforementioned negotiation of drug prices by the federal government. Trump pressed the pharmaceutical companies to bring drug manufacturing and production back to the United States. In return, Trump pledged to work to reduce corporate taxes, support deregulation, and streamline the FDA to expedite drug approvals. One can interpret those broad statements as a draft outline of the deal with pharma that will be struck by the Trump administration.
Where would such a deal leave the drug pricing issue? While Trump clearly expressed concern about high drug prices, the drug makers can offer him something else that he may want even more: jobs for U.S. workers that come from boosting production at existing plants and opening new plants on U.S. soil. Imagine the photo ops!
The Center of Medicaid and Medicare Service (CMS) continues to increase emphasis on care collaboration, ranging from Chronic Care Management (CCM) to the recent announcement from the US Surgeon General’s landmark report on alcohol, drug and health. Derived from many aspects in healthcare, the authors’ examine the challenges of integrating physical and behavioral healthcare, addressing the Care Collaboration Model outlined by CMS and the Surgeon General.
The author’s, beginning with the interdependency between physical and behavioral health, bring case scenarios supporting the challenges of today’s healthcare, and then introduce an innovative Health Collaborative Ecosystem addressing the many challenges of a care collaboration model.
Interdependency Between Mental and Other Chronic Disorders
Research has demonstrated bidirectional links between mental disorders and chronic conditions. Depression and anxiety are heightening the risks towards hypertension and diabetes. Depression roughly doubles the risk for a new coronary heart disease (CHD) event. We can go further on other mental disorders such as PTSD, drug addiction and alcoholism. Such interdependencies have limited solutions today due to the lack of a collaborative environment. We refer to this as a ‘revolving door care environment’, a vicious cycle compounding the effects of chronic and mental disorders.
A detox center can only retain the patient for detoxification for a limited time. Without collaborating with other behavioral services, the patient will inevitably return to the same habit – either drug addiction or alcoholism. Depression can stem from a social environment or from a recently developed chronic condition such as CHD.
The primary care provider will continue to address the chronic condition without the knowledge of what may actually feed into the patient’s chronic condition. It is yet another ‘revolving door’ for the physical care environment. Such interdependency requires a care collaborative environment between care providers.
Care Collaborative Model and Bidirectional Information Flow
A team-based care collaborative model uses a multidiscipline group of care providers supporting and implementing treatment with the patient at the center. A bidirectional information flow is an absolute must to put the model into realization and operation in healthcare institutes.
Today, healthcare lacks the support of a closed-loop system, one that emphasizes a bi-directional flow of information. Healthcare is muddled with reactive care, instead of preventive, anticipated care. It is that lack of prevention and anticipation that have an adverse impact on the overall healthcare cost and patient outcomes. EHR and EMR systems are the main ‘anchors’ of today’s health IT.
However, there are two EHR components that are non-starters: the boundary of the health institute and unidirectional systems. HIEs (Health Information Exchange) address EHR limitations with their capability to provide support across health institutes, but actually worsen the unidirectional character of the EHR. Neither EHR or HIE can address the requirements for a care collaborative model.
Reaching The State of Homeostasis As A Desired Patient Outcome
The objective is to improve patient outcomes, but how do you define a patient’s outcome?
Homeostasis is a biological term, referring to the stability, balance, or equilibrium within the body. Homeostasis is the process of maintaining a constant internal environment by providing the body with what is needed to survive for the well being of the whole. While disorders (physical or mental) reflect the abnormal condition of the body, homeostasis is the normal, stable and well-being state.
Each disorder is well documented with what would be a normal condition or the state of homeostasis. This state of homeostasis also deviates based on race, demographics, and above all, the relationship with other existing disorders afflicting the patient. It is then noted that each patient outcome requires a personalized state of homeostasis.
From the disorder, the process towards the state of homeostasis consists of genetics, nutrition, physical activity, mental health and an external environment. Genetics is the internal influencer in with medicine’s physical care plays a role in adjusting the disorder toward homeostasis. For healthcare, it is the care plan for a disorder.
The state of homeostasis should be used as the measure of a patient’s outcome, resulting from the care collaborative model addressing the integrated, coordinated care from multiple care providers.
Health Collaborative Ecosystem
The Health Collaborative Ecosystem is the delivery process that supports the care collaborative model, with the objective of bringing the patient to the state of homeostasis. This system would include all providers of health-related services to the chronically ill patient diagnosed with one or more of the designated chronic and debilitating diagnosis that utilize the most significant percentage of health care spending. Such a system would be:
Capable of integrating physical and mental care environments.
An integrated layer complementing (including EHR-agnostic) existing health IT infrastructures, supporting care activities beyond the brick and mortal walls of their facility or clinic.
Consensus among providers to standards of care and bidirectional information flow that encourages innovation, compliance with regulations, secures privacy and adopts a continuous process of improvements to better reach a patient’s state of homeostasis.
Why an Ecosystem?
An Ecosystem is a collective system, including a health IT solution and consulting guidance, and support, for hospital operations in order to maximize the benefits of care collaboration, through efficiency and scalability of a care providers’ bandwidth.
It is an Ecosystem because it must include an auditable compliance component to provide crucial measurements and enforce quality guidelines for the model according to hospital and clinic management.
It is an Ecosystem because it must include the ability to track and monitor progress towards the state of homeostasis for all attributes contributing the patient’s overall well being.
Case scenarios
As noted in one case study, Maria Viera, age 75, takes a dozen medications to treat her diabetes, high blood pressure, mild congestive heart failure, and arthritis. After she begins to have trouble remembering to take her pills, she and her husband visit her primary care physician to discuss this and a list of other worrisome developments, including hip and knee pain, dizziness, low blood sugar, and a recent fall. Maria’s primary care doctor spends as much time with her as he dares, knowing that every extra minute will put him further behind schedule. Yet despite his efforts, there is not enough time to address her myriad ailments. She sees several specialists, but no one talks to all her providers about her care, which means she may now be dealing with conflicting recommendations for treatment, or medications that could interact harmfully. As a result, Maria is at high risk for avoidable complications and potentially preventable emergency department visits and hospital stays.
The care team for the above patient would potentially consists of: a primary care provider (high blood pressure and care coordinator), a cardiologist (congestion heart failure), an endocrinologist (diabetes), dietician (diabetes), a rheumatologist (arthritis), physical and/or occupational therapists (arthritis, falls, hip and knee pain), and a psychologist or a psychiatrist (depression).
The above case brings challenges to the health care system on multiple fronts:
More time from primary care providers with limited result outcomes due to the lack of collaboration with other care providers, specialists and community services.
Potential conflicting recommendations for treatment due to the lack of coordination and bidirectional medical information flows from multiple care providers and specialists.
The patient’s risk for complications, emergency visits and hospital stays significantly increases.
As conditions worsen, the patient develops symptoms for behavioral health conditions.
Today’s solution for the above scenario is based on care management. The care manager would work with all care providers, manually “pulling and pushing” the patient’s medical conditions and updates to all involved care providers. Error prone, high cost, and low efficiency are some of today’s deficiencies for healthcare attempts in implementing the care collaborative model, outlined by CMS.
Net New Revenue Focusing on Preventive Care
This is the challenge of a ‘revolving door care environment’ in addressing the need for integration between physical and behavioral health services. The Health Collaborative Ecosystem is the answer for such a challenge.
However, to support such a revolution, healthcare, as an industry, needs to have the financial incentives. As stated in the introduction of this paper, CMS is not encouraging a transformation through financial incentives.
The authors’ propose a roadmap to roll out the Health Collaborative Ecosystem without upfront risks and budget planning, but to generate new revenue for the institutes. The implementation roadmap leverages these CMS initiatives:
Annual wellness visits
Chronic care management
Integration of physical and behavioral health through the care collaboration model
With the Health Collaborative Ecosystem’s objective is to create a patient state of homeostasis, rural and community hospitals and clinics can accomplish multiple goals – better services to the community, better defined patient outcomes and open new avenues for health services with behavioral health and filling the revenue gap.
Now that electronic health records have become the norm, healthcare providers — as well as healthcare systems and insurers — have access to unprecedented amounts of patient data. As a result, the practice of data mining, or analyzing data sets to identify trends and patterns, has become commonplace in healthcare, with the ultimate intent of improving patient care, improving efficiencies in the delivery of care, and reducing costs. Simply put, data mining has the potential to save lives and save money, but that doesn’t mean that it isn’t without risk.
As you might expect, using patient data for any purpose beyond providing care for the individual patient brings with it some tricky issues regarding privacy, and keeping the information from falling into the wrong hands. There are significant legal issues related to the use of patient data in data mining efforts, specifically related to the de-identification, aggregation, and storage of the data. Failing to take the appropriate steps when using personal health data as a tool for population health could lead to serious consequences, including a violation of HIPAA.
The question, then, is how to protect patient privacy while still gaining the insights that data mining can provide.
Protecting Patient Privacy for Data Mining
One of the major security concerns related to data mining is the fact that many patients don’t even realize that their information is being used in this way. Considering the way in which mined information can be used, this is of concern to many privacy advocates.
For example, in one noted example, Carolinas HealthCare, which runs more than 900 care facilities in the southern U.S., has purchased consumer data on more than two million people, which they use in algorithms to determine the risk for illness. The data includes purchase information collected from credit cards and consumer loyalty programs, as well as public records, to determine which people are at the most risk of getting sick. Providers can potentially use this information to remind patients to visit the gym more often, or encourage them to stop eating so much fast food. Other hospitals have used general demographic information about home and vehicle ownership or family makeup, to gain insight into a patient’s health and well-being, as well as identify potential barriers to care. However, what sets this type of data mining apart from healthcare data mining is that it’s data collected via other sources, and therefore not covered by HIPAA rules.
Still, many patients who have been contacted as a result of this type of data mining have noted that the practice feels intrusive. Even more intrusive is the potential for their personal health data to be used in this way, especially without their permission. Under HIPAA rules, data mining is a secondary, future use of health data, and thus requires the explicit permission of the patient before being used.
By the very definition, data mining is the process of looking for previously unknown patterns in data, so there is no way of knowing from the beginning what data is useful, or what relationships will be uncovered, meaning that there is potential for identifying information to be used or revealed. This highlights an important consideration when it comes to collecting and using personal information for data mining: Permission from the individual. Privacy advocates recommend offering patients the option to opt-in, opt out of specific uses, or opt-out entirely.
Running a healthcare facility is a herculean task even with the most experienced staff. Most studies on the state of healthcare industry decry the high cost of equipment maintenance and it is also the greatest challenge that every hospital administrator deals with. Breakdown of hospital equipment can lead to fatalities and this is why you need to leverage preventive maintenance software to avoid legal issues and costly repairs.
Computerized maintenance management system (CMMS) will help reduce hemorrhage of hospital revenues through unforeseen equipment breakdowns. This system is used to schedule preventive maintenance at the healthcare facility thus avoiding downtime of the machines. With this software, all of the hospital’s assets are tracked and monitored and all of this information is presented on one single dashboard. As the facility manager, you have instantaneous access to information about the condition of all the equipment. With such access to information the maintenance procedures are easier to execute, which saves the institution from financial loss and also improves the quality of patient care provided.
To appreciate why you should invest in such a maintenance system, consider the folowing benefits:
Improved Patient Care
The patients are the top priority in a healthcare facility and as such all efforts should be directed towards providing quality care. By adopting the CMMSsoftware, you will have preventive measures in place in case of equipment failure. The health of patients is in your hands and situations such as power outages and equipment failure must be averted, as they can result in fatalities. You are able to come up with contingency plans in case of emergencies and the system also helps in case of evacuations. By providing for real-time communication between members of staff, this software improves the level of service offered at the facility.
Improved Asset and Inventory Management
A vast healthcare facility receives lots of supplies daily, and these are crucial in offering appropriate health services. Tracking all these supplies manually is very tricky and tedious, but with an automated system you can keep track of what is available and what needs to be replenished, quite easily. You can also monitor which departments are consuming more supplies and make relevant decisions based on such information. This system also helps you keep track of the equipment in the facility. If there are any due repairs, it is easier to alert the concerned parties to avoid downtime.
Risk Assessment
A hospital environment provides unique challenges and risk assessment is crucial to avoid accidents. The best maintenance management software also enables you to assess the potential risks in any project and equipment. By receiving such information beforehand, you are able to preempt any risks and avoid accidents. You can also carry out quality safety inspection to ensure every department is prepared for any unanticipated risks.Continue Reading
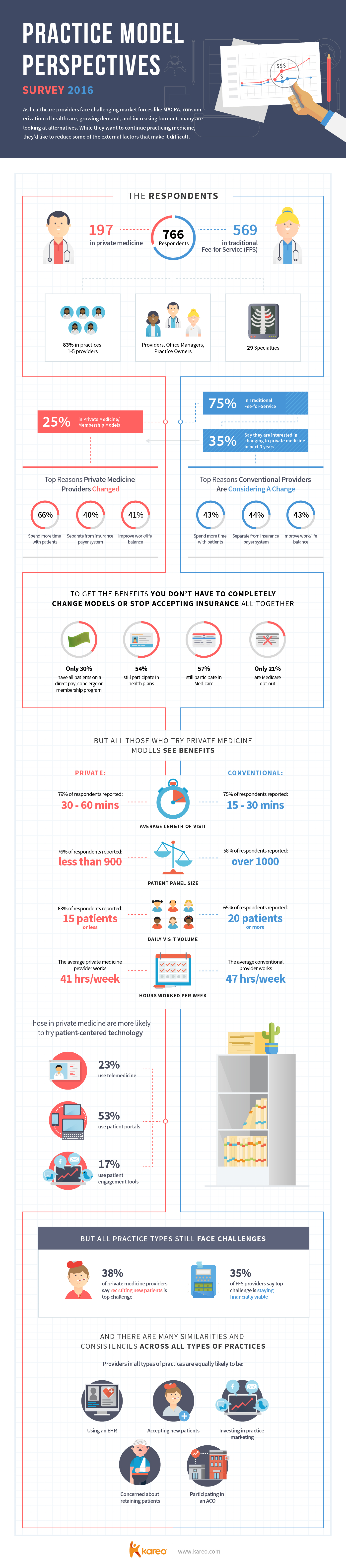
Healthcare providers continue to face new and growing challenges across the marketplace. From the release of the MACRA final rule to the consumerization of healthcare, there is a lot to balance and manage. It can be hard to keep up while also trying to provide quality care and get paid. As a result, providers continue to look at alternate payment models according to a new survey from Kareo and the American Academy of Private Physicians (AAPP).
The survey shows that 25 percent of practices are now using some kind of direct pay, concierge, or other membership model in their practice. This number stayed steady from the 2015 study to the 2016 study. Most do not have all their patients on one of these models, but 30 percent have completely transitioned their practice. The results show that many practices are testing these models while still offering patient other options like traditional fee-for-service. This may suggest that physicians want to see how successful the models before shifting their entire practice.
Another 35 percent of providers say they are considering a change in part or in whole to an alternate model like direct pay or concierge. The reasons are consistent with the results from the 2015 survey. The top reason cited was to separate from the insurance payer system, closely followed by spending more time with patients and improving work/life balance.
The survey indicates that those physicians who do switch see improvements in those areas. Physicians using direct pay, concierge or another membership model spend more time with patients, see fewer patients each day at longer visits, and work fewer hours than their fee-for-service counterparts.
This infographic shows the details of both the differences and the similarities when physicians use private pay models versus fee-for-service models.



 Now that electronic health records have become the norm, healthcare providers — as well as healthcare systems and insurers — have access to unprecedented amounts of patient data. As a result, the practice of data mining, or analyzing data sets to identify trends and patterns, has become commonplace in healthcare, with the ultimate intent of improving patient care, improving efficiencies in the delivery of care, and reducing costs. Simply put, data mining has the potential to save lives and save money, but that doesn’t mean that it isn’t without risk.
Now that electronic health records have become the norm, healthcare providers — as well as healthcare systems and insurers — have access to unprecedented amounts of patient data. As a result, the practice of data mining, or analyzing data sets to identify trends and patterns, has become commonplace in healthcare, with the ultimate intent of improving patient care, improving efficiencies in the delivery of care, and reducing costs. Simply put, data mining has the potential to save lives and save money, but that doesn’t mean that it isn’t without risk.