While interoperability has always been one of healthcare’s greatest pain points, the last year or so has emphasized these challenges with the rising demand for data integration and information sharing. The pandemic has required high volumes of data integration, and it’s been difficult for organizations to adapt and respond in an effective and efficient way.
These challenges were further compounded this year with the impending ONC/CMS information blocking rules. With the previous administration’s focus on improving interoperability coinciding with a global health emergency, healthcare organizations had more on their plate than ever. As we look to the future of healthcare in a post-COVID environment, and to the new administration and its healthcare goals, what can healthcare organizations expect?
Healthcare organizations must remain flexible and optimize the organization to be as adaptable as possible. In our interview with Ivan, we explore what healthcare organizations should know about the information blocking rules and the new administration, what is really at the root of the healthcare interoperability problem, and best practices healthcare leaders can employ to set their organizations up for success now and in the future.
How would you define the healthcare interoperability problem?
Interoperability is an evergreen problem across the healthcare industry. As we continue to innovate new capabilities and concepts, we are also constantly expanding our interoperability needs. In a way, interoperability isn’t a problem to be solved. It’s an ongoing practice that has to evolve alongside our other capabilities. For example, there was a time not long ago when social determinants of health (SDoH) were not on anyone’s radar, but as SDoH became more important to healthcare practitioners, it was clear we needed not only to track and store SDoH-related data but also exchange that data across different software systems and organizations. The goal of HL7’s Gravity Project is to build out the standards for exchanging SDOH data using FHIR.
2020 was a tough year in healthcare. The demand for data integration was up, exposing the dire need for better data integration across the healthcare ecosystem. In a world where interoperability wasn’t an issue, how could the pandemic have looked different?
The bad news is that we live in a world where the most reliable COVID vaccination records are stored on paper cards and interoperability is achieved by the patient themselves carrying the card from place to place. In an ideal world, the vaccination would come with an electronic record that the patient could capture on their mobile device and upload to their doctor’s EHR system, their employer’s HR system, and any other third party that needed to see proof of vaccination.
Although we’ve fallen far short of the ideal state, there are some interoperability bright spots to be happy about. For example, we’ve been able to onboard many new sources of lab result data and integrate that into public health departments. This has not always been easy, but because of the ONC’s prior work on the Promoting Interoperability program, we already had agreed-upon standards and an infrastructure in place to move the data from location to location.
By Drew Ivan, chief product and strategy officer, Lyniate.
It is becoming increasingly popular to move healthcare outside of the clinic and into the community and the home with the use of telemedicine platforms, apps, and other digital means — and the coronavirus pandemic has dramatically accelerated that trend. Counterintuitively, this healthcare crisis has the potential to attenuate the relationship between the patient and the healthcare system, putting provider organizations at increased risk from “digital disruptors” like Amazon, Google and Apple, whose ambitions to take over consumer relationships in healthcare are stronger than ever.
As patients re-orient during the pandemic around other points of care (hospitals, urgent care, pharmacy, etc.), the relationship patients have with their PCPs (which is one of the health system’s biggest and most meaningful advantages against the advancement of healthcare disruptors), can lose value to the consumer. As such, it behooves health systems — who are understandably all hands on deck working to address the COVID-19 crisis today — to be giving serious consideration to ways of fending off digital disruptors as their big challenge in a post-COVID-19 world.
This means focusing on leveraging the unique strengths and assets they have and getting smart about aggregating and using the disparate consumer/patient data sets they manage, to deliver a consumer experience only they can provide.
Digital disruptors excel at delivering exceptional digital customer experiences by using the massive data sets at their disposal that render rich insights into customer trends, needs, behaviors, preferences, proclivities, etc. With that said, hospitals and health systems have an advantage in their exclusive access to patient data and their in-depth medical knowledge.
Health systems need to thoughtfully but aggressively leverage these advantages if they want to successfully retain primacy in the consumer’s healthcare brand relationships. With non-emergent care rapidly shifting to the digital space, digital brands have a golden opportunity to disrupt the traditional patient-health system relationship should provider organizations miss the opportunity to reinforce those relationships by delivering much more personalized digital interactions.
It’s important to remember that healthcare organizations do not need to match the digital sophistication of the big data-driven consumer tech giants. They just need to use what they already know about patients, communities and medicine to create the kinds of experience for patients that only they can.
As hospital leaders aim to protect their organizations from digital disruptors in the post-coronavirus aftermath, these three considerations should be top of mind:
Healthcare is home to some of the most mind-blowing technological advances when it comes to diagnostics and therapies. At the same time, the healthcare system is responsible for many of the most head-scratching operational difficulties related to standard IT processes, such as those involved with moving data from one system or site to another. The same industry that successfully deploys remote-controlled surgery robots to heal a patient also struggles to send a discharge summary to a physical therapist for the same patient.
How can we explain this apparent paradox?
A Model of Interoperability
The simple answer is that interoperability in healthcare is a journey, not a destination. The question “why haven’t we solved interoperability?” assumes that interoperability is a one-time problem, when in fact the systems, standards, and data flows that constitute interoperability are constantly changing as the underlying patterns of treatment and reimbursement change.
Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine[1].
In the center, provider, or organizational, interoperability indicates data flows within a single organization, typically a hospital or hospital system. This has historically been dominated by HL7 v2 transmitted over a TCP connection on a private network, although other standards and technologies are also used.
At the top, community, regional, and national cross-organizational Interoperability refers to communication of healthcare data across different organizations, for example ACOs, HIEs, and provider-to-payer data flows. In this part of the model, we often see IHE style integrations that exchange entire patient records in a single, secure transaction over a public network.
At the bottom, the Internet of Medical Things (IoMT) is divided into two parts: medical device interoperability, which concerns devices used in a clinical setting, and consumer device interoperability – commercially available devices marketed directly to consumers, such as fitness devices and in-home monitors.
On the left, healthcare IT vendors need to enable their products to interoperate at different levels of the interoperability model, depending on which markets they serve. For example, an EHR vendor will need its product to send and receive HL7 v2 messages in order to participate in the organizational interoperability space.
On the right, we are seeing an increased demand for patient or consumer access to their data, whether it is from a fitness device, a hospital’s EHR, or a payer’s disease management system. Integration in this box is often accomplished using APIs, including FHIR.
By Drew Ivan, EVP of product and strategy of Rhapsody.
Drew Ivan
It was generally recognized by 2009 that the health care industry was long overdue when it came to adopting electronic systems for storing patient data. At the time, hospital adoption of electronic health record (EHR) systems was at about 10 percent while electronic record keeping was commonplace in most other industries. EHR technology was widely available, yet doctors and hospitals were still using paper charts.
The HITECH Act of 2009 was part of a broader stimulus package that financially nudged hospitals and eligible professionals to adopt and use EHRs. The meaningful use incentive program began a national, decade-long project to adopt, implement, and optimize EHR software. The program was a huge success, judged by the most obvious metric, EHR adoption. Today, nearly 100 percent of hospitals are using electronic health records. This means that records are safe from physical damage, far easier to analyze and report on, and – in theory at least – easier to transfer from one provider to another.
However, when viewed through the lens of return on investment, the success is less impressive. The federal government has spent $36 billion to encourage providers to adopt EHR systems but the industry has spent far more than that to procure, implement and optimize the software. Yet, hospitals are seeing reduced productivity, doctors face a huge documentation burden, and interoperability remains an unsolved problem. The first two problems are the consequence of workflow changes brought on by the EHR systems, but interoperability roadblocks ought to have been eliminated by implementing EHR systems, so why is it still so difficult to transfer records from one provider to another, or from a provider to the patient?
Health IT experts generally consider three categories of obstacles to interoperability:
Business disincentives: allowing medical records to move to a different provider makes it easier for patients themselves to move to another provider, and helping customers switch health care providers is contraindicated by usual business practices (even though HIPAA states that patients are entitled to receive copies of their medical records and may direct copies of their records to be sent elsewhere.)
Technical challenges: Meaningful use set a fairly low bar for cross-organizational data exchange requirements, and it did little to ensure that EHR systems could understand data sent from another system. Although these problems are largely resolved today, there is still the impression that “interoperability is a hard technical problem”.
Network effects: point-to-point connections between providers are impractical, but the network approach also has its drawbacks. The assortment of HIEs and national interoperability initiatives is huge and confusing, and it’s not obvious which network(s) an organization should join.
There may have been an assumption that when medical records moved from paper to electronic format they would immediately become more interoperable, but by 2016, the level of interoperability was far below what patients and regulators expected. As a result, the 21st Century Cures Act of 2016 was passed by Congress and signed into law by the outgoing Obama administration. The law’s scope included a number of health care priorities, including a patch for the interoperability gap left by Meaningful Use. Cures explicitly forbids providers, technology vendors, and other organizations from engaging in “information blocking” practices.
Earlier in 2019, the Office of the National Coordinator for Health IT (ONC) issued a notice of proposed rulemaking (NPRM) that defined exactly what is (and what is not) meant by “information blocking.” Once adopted, the expectation will be that a patient’s medical records will move according to the patient’s preferences. Patients will be able to direct their data to other providers and easily obtain copies of their data in electronic format.
The Department of Health and Human Services (HHS) filed its annual year-end report to Congress at the start of 2019. The 22-page report summarized nationwide trends in health information exchange in 2018, including the adoption of EHRs and other technologies that support electronic access to patient information. The most interesting takeaway has to do with the ever-elusive healthcare interoperability.
According to the report, HHS said it heard from stakeholders about several barriers to interoperable access to health information remain, including technical, financial, trust and business practice barriers. “These barriers impede the movement of health information to where it is needed across the care continuum,” the report said. “In addition, burden arising from quality reporting, documentation, administrative, and billing requirements that prescribe how health IT systems are designed also hamper the innovative usability of health IT.”
To better understand these barriers, HHS said it conducted multiple outreach efforts to engage the clinical community and health IT stakeholders to better understand these barriers. Based on these takeaways, HHS said it plans to support, through its policies, and that the health IT community as a whole can take to accelerate progress: Focus on improving interoperability and upgrading technical capabilities of health IT, so patients can securely access, aggregate, and move their health information using their smartphones (or other devices) and healthcare providers can easily send, receive, and analyze patient data; increase transparency in data sharing practices and strengthen technical capabilities of health IT so payers can access population-level clinical data to promote economic transparency and operational efficiency to lower the cost of care and administrative costs; and prioritize improving health IT and reducing documentation burden, time inefficiencies, and hassle for health care providers, so they can focus on their patients rather than their computers.
Additionally, HHS said it plans to leverage the 21st Century Cures Act to enhance innovation and promote access and use of electronic health information. The Cures Act includes provisions that can: promote the development and use of upgraded health IT capabilities; establish transparent expectations for data sharing, including through open application programming interfaces (APIs); and improve the health IT end user experience, including by reducing administrative burden.
“Patients, healthcare providers, and payers with appropriate access to health information can use modern computing solutions (e.g., machine learning and artificial intelligence) to benefit from the data,” HHS said in its report. “Improved interoperability can strengthen market competition, result in greater quality, safety and value for patients, payers, and the healthcare system generally, and enable patients, healthcare providers, and payers to experience the promised benefits of health IT.”
Interoperability barriers include:
Technical barriers: These limit interoperability through—for example—a lack of standards development, data quality, and patient and health care provider data matching. Addressing these technical barriers by coordinating to establish the technological foundation for standardizing electronic health information and by promoting exchange of that information can considerably remove these barriers.
Financial barriers: These relate to the costs of developing, implementing, and optimizing health IT to meet frequently changing requirements of health care programs. The cost to adjust health IT to meet these requirements can impact innovation and the timeliness of technical upgrades. Specific barriers include the lack of sufficient incentives for sharing information between health care providers, the need for enhanced business models for secondary uses of data, and the current business models for health systems or health care providers that do not adequately focus on improving data quality.
Trust barriers: Legal and business incentives to keep data from moving present challenges. Health information networks and their participants often treat individuals’ electronic health information as an asset that can be restricted to obtain or maintain competitive advantage.
Elsewhere, the Center for Medical Interoperability, located in Nashville, Tenn., is an organization that is working to promote plug-and-play interoperability. The center’s members include LifePoint Hospitals, Northwestern Memorial Healthcare, Hospital Corporation of America, Cedars-Sinai Health System, Hennepin Healthcare System, Ascension Health, Community Health Systems, Scripps Health, and UNC Health Care System.
Its mission is “to achieve plug-and-play interoperability by unifying healthcare organizations to compel change, building a lab to solve shared technical challenges, and pioneering innovative research and development.” The center stressed that the “lack of plug-and-play interoperability can compromise patient safety, impact care quality and outcomes, contribute to clinician fatigue and waste billions of dollars a year.”
More interoperability barriers identified
In a separate study, “Variation in Interoperability Among U.S. Non-federal Acute Care Hospitals in 2017,” showed additional difficulty integrating information into the EHR was the most common reason reported by hospitals for not using health information received electronically from sources outside their health system. Lack of timely information, unusable formats and difficulty finding specific, relevant information also made the list, according to the 2017 American Hospital Association (AHA) Annual Survey, Information Technology Supplement.
Among the explanations health systems provided for rarely or never using patient health information received electronically from providers or sources outside their health system:
Difficult to integrate information in EHR: 55 percent (percentage of hospitals citing this reason)
Information not always available when needed (e.g. timely): 47 percent
Information not presented in a useful format: 31 percent
Information that is specific and relevant is hard to find: 20 percent
Information available and integrated into the EHR but not part of clinicians’ workflow: 16 percent
Hospitals, when asked to explain their primary inability to send information though an electronic exchange, pointed to: Difficulty locating providers’ addresses. The combined reasons, ranked in order regardless of hospital classification (small, rural, CAH or national) include:
Difficult to find providers’ addresses
Exchange partners’ EHR system lacks capability to receive data
Exchange partners we would like to send data to do not have an EHR or other electronic system to receive data
Many recipients of care summaries report that the information is not useful
Cumbersome workflow to send the information from our EHR system
The complexity of state and federal privacy and security regulations makes it difficult for us to determine whether it is permissible to electronically exchange patient health information
Lack the technical capability to electronically send patient health information to outside providers or other sources
Additional Barriers
The report also details other barriers related to exchanging patient health information, citing the 2017 AHA survey:
Greater challenges exchanging data across different vendor platforms
Paying additional costs to exchange with organizations outside our system
[Need to] develop customized interfaces in order to electronically exchange health information
“Policies aimed at addressing these barriers will be particularly important for improving interoperable exchange in health care,” the report concluded. “The 2015 Edition of the health IT certification criteria includes updated technical requirements that allow for innovation to occur around application programming interfaces (APIs) and interoperability-focused standards such that data are accessible and can be more easily exchanged. The 21st Century Cures Act of 2016 further builds upon this work to improve data sharing by calling for the development of open APIs and a Trusted Exchange Framework and Common Agreement. These efforts, along with many others, should further improvements in interoperability.”
What healthcare leaders are saying about interoperability
While HHS said it conducted outreach efforts to engage health IT stakeholders to better understand these barriers, we did too. To further understand what’s currently going on with healthcare interoperability, read the following perspectives from some of the industry’s leaders. If there’s something more that you think must be done to improve healthcare interoperability, let us know:

 It is becoming increasingly popular to move healthcare outside of the clinic and into the community and the home with the use of telemedicine platforms, apps, and other digital means — and the coronavirus pandemic has dramatically accelerated that trend. Counterintuitively, this healthcare crisis has the potential to attenuate the relationship between the patient and the healthcare system, putting provider organizations at increased risk from “digital disruptors” like Amazon, Google and Apple, whose ambitions to take over consumer relationships in healthcare are stronger than ever.
It is becoming increasingly popular to move healthcare outside of the clinic and into the community and the home with the use of telemedicine platforms, apps, and other digital means — and the coronavirus pandemic has dramatically accelerated that trend. Counterintuitively, this healthcare crisis has the potential to attenuate the relationship between the patient and the healthcare system, putting provider organizations at increased risk from “digital disruptors” like Amazon, Google and Apple, whose ambitions to take over consumer relationships in healthcare are stronger than ever.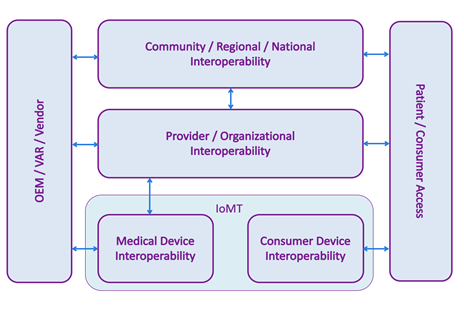 Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine
Interoperability today spans more systems and settings than ever before, and “interoperability” means different things to different audiences, so it’s worth taking a moment to ponder the modern interoperability landscape. The following model is an expansion of one suggested by the National Academy of Medicine
 The Department of Health and Human Services (HHS) filed its annual year-end
The Department of Health and Human Services (HHS) filed its annual year-end