Visiting nurses are valued for their caring and compassionate nature. Their valuable skillset makes a difference in the well-being of their patients and the lives of patients’ families. However, they face unique challenges amid the coronavirus as patients and staff are concerned about receiving in-home care during this time. Bringing healthcare to the home is no easy task.
As NAHC President William A. Dombi stated, “Home care and hospice nurses, therapists, aides, and other providers who choose to use their lives to serve our country’s aged, disabled, and dying. This noble work deserves our recognition and praise.”
Home health agencies are on the front line amid the coronavirus pandemic. A recent Home Care Association of New York State (HCA-NYS) survey found that nearly half of agencies in the survey said they have experienced patients or family members refusing entry of home care personnel. “Different states and regions are at different stages in surveillance and monitoring,” Roger Noyes, director of communications at HCA-NYS, told Home Health Care News.
“This speaks to some very important educational and outreach needs to reassure patients and to ensure that vital care can be delivered,” Noyes said. In addition to patients’ hesitation to let nurses into their homes for in-person visits, many patients are already quarantined, sheltering in place, or social distancing. And, some patients are denying service because they appreciate their nurses so much that they do not want to risk getting their nurse sick in-person. Concurrently, the nurses themselves might also be wary of conducting in-person visits as they might not have sufficient protective gear and/or fear the risk of infection.
Agencies are implementing telehealth/virtual care to preserve their patients, their staff and their limited supplies. Technology can help agencies’ staff continue what they do – provide compassionate and critical care – and “be present” with their patients as much as possible. With technology, agencies can safely continue the delivery of care during this time and quickly communicate critical updates as needed. The technology helps home healthcare agencies:
Conduct virtual visits with patients to safely ensure continuity of care
Send out critical COVID-19 updates and self-care tips
Send condition-specific messages to improve ongoing adherence
Provide virtual access to their staff which helps nurses address patients’ emerging concerns and also alleviate patients’ loneliness while being socially isolated
With virtual visits, agencies are kept abreast of the realities of the patient’s home environment and their available resources (financial, food, social, etc.). Staff can continue to monitor their patients’ day-to-day situation and individualize the care (and conversation) to the “new normal” for the at-home patient.
OneBlood, the not-for-profit blood center serving Florida and other parts of the southeastern United States, will soon begin collecting plasma from people who have recovered from the coronavirus so it can be transfused to people with life-threatening coronavirus infection in hopes of aiding their recovery.
The experimental treatment is approved by the FDA to be used on an emergency basis and is called “COVID-19 convalescent plasma.”
People who recover from coronavirus infection have developed antibodies to the virus that remain in the plasma portion of their blood. Transfusing the plasma that contains the antibodies into a person still fighting the virus can provide a boost to the patient’s immune system and potentially help them recover.
OneBlood is working closely with the Florida Department of Health to identify people who have recovered from COVID-19 to be potential donors. In addition to local efforts, OneBlood is also cooperating with the federal government and anticipates participating in a national-level initiative to be able to provide convalescent plasma when and where it is needed.
OneBlood is working quickly to implement the new protocols to meet the FDA criteria for COVID-19 convalescent plasma. OneBlood plans to begin collecting plasma from qualified donors in the coming weeks and also plans to start offering the therapeutic agent to hospitals to treat severely ill coronavirus patients. As one of the largest blood centers in the country, OneBlood already has the technology in place to be able to collect, test and process plasma from donors.
The potential donors will need to meet all the usual screening criteria for blood donation, plus pass additional FDA criteria, including:
COVID-19 convalescent plasma must only be collected from recovered individuals if they are eligible to donate blood
Required testing must be performed and the donation must be found suitable
Prior diagnosis of COVID-19 documented by a laboratory test
Complete resolution of symptoms at least 14 days prior to donation
Have a negative result for COVID-19
Meet all standard FDA blood donation requirements
As with all transfusions, the donor and the patient will need to have compatible blood types
In addition, the recipients of the plasma will also have to meet FDA criteria in order to qualify to receive this therapy for treating life-threatening COVID-19. (Click here for FDA report).
By Brian Kirkendall, vice president of product management, Digi International.
Brian Kirkendall
In 1847, Hungarian physician Ignaz Semmelweis theorized that hand washing could limit the occurrence of puerperal fever among new mothers. But despite the obvious success of his proposal, he faced significant opposition from his colleagues in the medical community, many of whom flatly rejected his theory.
Of course, today more than ever, we’re acutely aware of the importance of Semmelweis’ game-changing understanding of hand washing, and we are tracking it more closely than ever before. Fortunately, our modern healthcare industry is equipped with far more than mere chlorinated lime solutions that our forefathers had in the 19th century. And the Internet of Things (IoT) is stepping in to support healthcare providers with breakthroughs that can enhance our preparedness to fight and prevent infections and mitigate the spread of contagions such as COVID-19.
Can IoT help keep us safe?
The healthcare industry has long been a careful early adopter of lifesaving and life changing innovations, so it comes as no surprise that the IoT has made steady inroads into all types of clinical settings: doctors’ offices, hospitals, clinics, ambulances and more. From patient-connected devices for accurate and vigilant patient care to medical equipment such as pain medication management and hygiene monitoring devices, the IoT is transforming almost every area of healthcare delivery.
The IoT’s compelling combination of compact and low-cost hardware and software creates a far-reaching impact for caregivers and patients alike in the form of improved accuracy, greater efficiency, lower costs, and enhanced health and safety.
Today, one application that’s gaining wide notice is the use of wireless technology to monitor and report on hygiene compliance in the medical industry. The implementation of wireless sensors and flexible gateways are bringing unprecedented precision, including temperature and pressure monitoring in surgical suites, monitoring cryogenic environments or something as routine – but life-saving – as hand hygiene.
A real-life use case: Sanitize your hands
We usually think hospitals are some of the most hygienic places of all. However, given the high traffic of sick people, hospitals that aren’t rigorous and vigilant can be home to greater infectious risks. Due to the number of immunocompromised patients present, hospitals face an ongoing mission-critical challenge to prevent the spread of bacteria and infectious diseases. Long before the COVID-19 global pandemic, the Clean Hands Safe Hands (CHSH) initiative recognized this importance of this issue and promulgated hand washing strategies that use wireless technology to help healthcare institutions promote health and safety.
As simple as it sounds, in a hectic environment like a healthcare facility, simple vigilance in washing hands can be the No. 1 factor in keeping medical workers and patients safer. What a better way to improve hand cleanliness than by providing hospitals with internet-connected hand-sanitizing stations?
As COVID-19 closes in the on U.S., the need for longitudinal health data and interoperability have never been greater. Providers need access to the full picture of every patient they treat, and epidemiologists need to consolidate data from multiple sources to track the spread of the disease and determine where more aggressive containment strategies need to be employed.
For many organizations already overwhelmed, fragmented systems lead to an infrastructure bottleneck, resulting in degraded data quality, gaps in care coordination, medical errors and burdensome workflows. Lack of comprehensive medical data impairs a provider’s ability to know how many people have the virus, the geographical location of confirmed cases, and the effectiveness of treatment.
Even as capacity restrictions force organizations to work without barriers—via drive-thru screenings, make-shift tents or by way of telehealth—real-time access to data can help streamline care management, whether fast tracking admissions or empowering patients at home through online portals.
Here are just five ways data interoperability plays a pivotal role in addressing the epidemic:
Coordination of Care: COVID-19 provides a sobering reminder of just how dire an integrated, scalable and interoperable healthcare infrastructure is. Coordination among first responders, public health officials, labs, acute and post-acute facilities will be critical to efficiently deal with the explosion of cases. Insurers will also be a key player of the care coordination team as to not slow down or hold up prior authorizations and patient discharges. Access to information about hospitalizations and test results among healthcare participants will be vital for enhanced continuity of care across settings and transitions. Real-time data afforded by interoperability bypasses the need for phone calls and faxes, which create delays and information inaccuracies.
Patient Identification: A complete view of one’s medical history can be a matter of life or death in the face of COVID-19. Bringing disparate medical records together into a cohesive story enables those on the frontlines insight into an individual’s pre-existing medical conditions, medications, allergies, etc. to make the most informed decisions under insurmountable circumstances. Patient demographics and data standardization play a huge role. Accurate patient identification ensures data about an individual is correctly linked, updated and shared, for improved clinical decision-making and enhanced care quality and safety. As health officials look to track and predict the spread of the virus. A complete view of the patient population can only be done with a firm understanding of the patient’s identity, and the key relationships the patient has to their next of kin and to their providers of care.
In this, the day and age of the global coronavirus outbreak, the job of the medical translator and interpreter has never been more relevant. Resolving this global crisis involves a great deal of research and analysis, much of it in the form of clinical trials. All of the requisite research and analysis must not only be reported and published but accurately documented as well. Once all of the research from the clinical trials has been completed, the information must be made readily available.
The document translation must be completed by certified medical translators and disseminated globally in order for the research to be relevant and helpful. This is an absolutely crucial role during any medically related global crisis but the medical translation of the clinical trial documentation will ultimately be the key to bringing the COVID-19 global pandemic to a successful conclusion before it can get any worse for the people of the world.
In tandem with the need for medical translation is the localization of clinical trials, which requires additional paperwork that the medical translator must make accessible to the world.
Document Requirements for Domestic and International
According to the National Institute of Health, “One of the most common inspection findings in investigator site inspections is lack of reliable, accurate and adequate source documentation. This also happens to be the most common pitfall identified during sponsor audits. The importance of good documentation practice needs to be emphasized to investigator sites to ensure that the study results are built on the foundation of credible and valid data.”
One of the biggest concerns during the current global medical crisis is that many of the clinical trials will not be properly published at all. Of those that are, many will suffer due to the improper documentation and document recordings, and all this before medical document translation begins. Among the biggest culprits of under-reporting, clinical trials were many academic institutions where certified medical translators should be readily available, and clinical trial document requirements should not be a challenge.
A study from the US Food and Drug Administration which is responsible for the oversight and investigation of Clinical Trials in the United States, inadequate documentation records were one of the top causes of clinical trials being brought into question or having them dismissed completely.
Clinical Trial Audits were most commonly required according to the FDA because of the following reasons:
failure to follow the investigational plan (34%)
inadequately informed consent form (28%)
inadequate/inaccurate records (27%)
The amount of documentation required to conduct a clinical trial is overwhelming on the best of days. Every one of the documents is absolutely relevant to the successful conclusion of the clinical trials being conducted by medical researchers.
This is especially true in terms of the current global Covid-19 pandemic. In terms of global clinical trials, translation services should work in support of the global effort, though this also requires that all of the documentation is in order, to begin with. Further, it relies on medical researchers working with a certified medical translation agency that also has the capacity to integrate and implement successful localization strategies to ensure the accuracy of the medical translations before they are distributed globally.
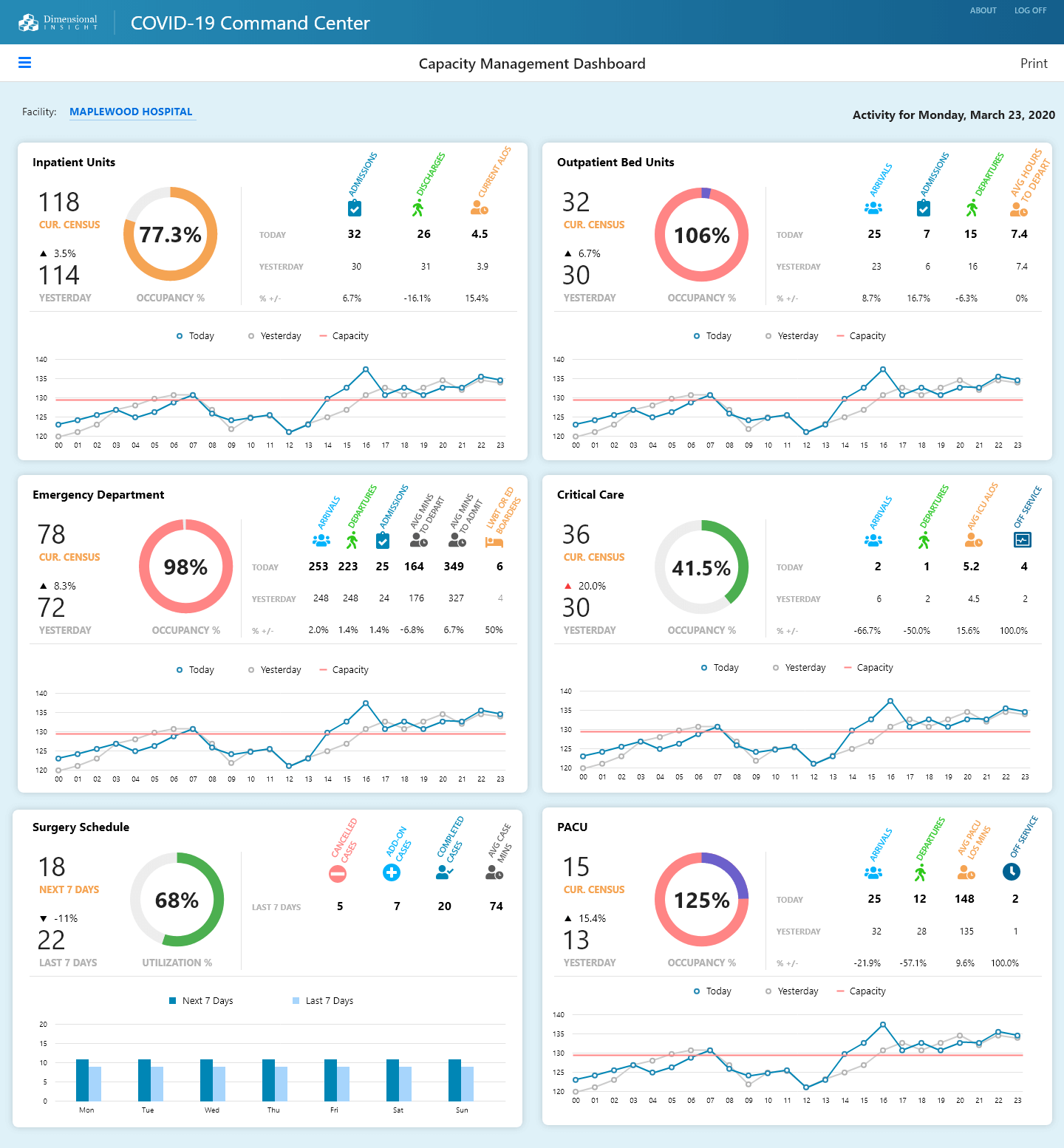
Dimensional Insight, maker of Diver Platform, the 2020 Best in KLAS healthcare business intelligence/analytics platform, today announced it is providing a complimentary* COVID-19 toolkit to healthcare providers.
This kit will provide critical measures or KPIs that hospitals and health systems need to track to better manage their COVID-19 patients, as well as the rest of their patient population. It will also include a capacity management dashboard that displays these current measures in an easy to understand format. In addition, the toolkit will include the logic to implement COVID-19 specific measures based on criteria provided by the CDC. This will result in better, more informed decisions in order to improve patient outcomes.
“As healthcare providers mobilize in their response to the COVID-19 pandemic, their data is an important guide in helping them understand where their resources are being used and what their capacity is as new patients come in,” says Fred Powers, CEO and co-founder of Dimensional Insight. “We are glad to share our expertise with healthcare organizations and provide this toolkit to them when it’s needed most.”
Some of the measures that the new COVID-19 toolkit will contain are related to:
COVID-19 specific (Confirmed COVID-19 cases, Potential COVID-19 cases, COVID-19 ALOS)
Inpatient Units (Census, Occupancy %, Admissions, Discharges, ALOS)
Outpatient Units (Census, Occupancy %, Arrivals, Admissions, Departures, Average Hours to Depart)
Emergency Department (Census, Occupancy %, Arrivals, Departures, Admissions, Average Minutes, LWBT)
Critical Care (Census, Occupancy %, Arrivals, Departures, Average ICU ALOS, Off service)
Surgery Schedule (Utilization %, Cancelled Cases, Add-On Cases, Completed Cases, Average Case Minutes)
PACU (Census, Occupancy %, Arrivals, Departures, Average PACU LOS Minutes, Off service)
Response from Oliver Lignell, vice president, virtual health, AVIA
Providers have a new tool to help them combat COVID-19: digital. Health systems are proactively leveraging digital assets to help triage, navigate, and treat cases in ways that address concerns and also reduce the spread of the virus to other patients and providers.
Virtual assistants and chatbots can help consumers explore symptoms, accurately triage their needs, and navigate them to the appropriate site of care. These solutions can both reduce consumer worries and potentially inappropriate use of EDs and urgent care clinics.
Virtual visits are another critical digital tool because they allow patients to complete a visit from the safety and comfort of their home without exposing them to crowded and potentially infectious clinical locations and, just as importantly, reduces wait times and crowds at in-person care sites.
Asynchronous virtual visits (store and forward, text/chat) can also be an important (and low-cost) solution. Consumers can initiate a low acuity visit on-demand, when convenient, ensuring their concerns are addressed when desired – with the added benefit of decreasing wait times, creating a more efficient patient flow, and freeing up provider capacity. Such solutions further reduce the pressure on health systems while improving the responsiveness to patients.
Response from Andrea Tait, vice president of Client Value, Orion Health
Digital tools can play a key role as healthcare providers across the globe struggle to maintain the health of their workforce and the capacity of their organizations. Pandemic response is best supported through triaging, testing and treating the affected. Tools like public-facing screeners, pandemic information sites and chatbots can help evaluate millions of people with little to no clinician support.
By triaging individuals, tools like remote patient monitoring and telehealth can be used to monitor patients from their homes and assure others that sheltering in place is sufficient. Remote monitoring tools allow clinicians to monitor more patients and make decisions about who may require testing. Designated testing sites minimize the need for direct interaction between healthcare providers and patients, preserving both the health and capacity of health service providers.
Integrated care pathways and telehealth tools can help clinicians treat more patients at home and discharge those in hospitals who may be safer receiving treatment for other conditions remotely, all while minimizing their own risk. Home and community delivered care is an increasingly essential component of healthcare system sustainability. Now, more than ever, these tools and strategies are fundamental to the future of the healthcare system.
Digital solutions can be employed in seemingly non-traditional ways to both prepare and respond to the impact of the coronavirus. For healthcare organizations, traditional pre-access telephone dialing metrics can be modified. Hospital registration staff, in addition to financial guidance and scheduling, can screen patients for COVID-19 and obtain additional clinical information in advance of arrival.
By identifying potentially infected patients, even before they enter the hospital, hospitals and clinics are able to communicate effectively within the facility and plan for appropriate patient care, monitor and manage potential for healthcare personnel COVID-19 exposure, and inhibit the spread of the disease both within the facility and community.
Equally important and sometimes forgotten, back-end services provided by both hospital staff and revenue cycle vendors yields the same patient communication opportunities. Discharged patient follow up and screening post-discharge keeps the patients connected and engaged with the hospital as well as preserves an open communication line between the hospital and discharged patient.
Response from Matthew A. Michela, president and CEO, Life Image
The coronavirus has manifested the importance of digital solutions and interoperability in a heightened way. The lack of digital connections to community referral sites will impact the safety of patients and healthcare staff. It is imperative during this public health crisis that attending healthcare workers have as much relevant clinical data in advance as possible through digital connections.
Unfortunately, many healthcare organizations are still deploying outdated technology, such as imaging CDs, and the last thing a provider or hospital should want is a patient who is symptomatic or potentially a carrier of a virus to show up with a CD in hand. This presents a problem on multiple levels, from the lack of care coordination to the risk of disease spread.
The technology is available and many large health systems are set up to support digital exchange, so they need to mandate protocols to exchange information in this manner. In the same way that the public is asked to wash their hands and frontline workers are urged to wear masks, healthcare professionals should insist that medical data is received digitally for fast, efficient care.
As we face the COVID-19 pandemic, it is important for hospital organizations to ensure information is delivered in real time, accurately, and highly customized to the intended audience (patients, visitors, clinicians, etc.). It can be beneficial for hospitals to automatically deliver COVID-19 patient education videos tailored for each patient’s demographics, language, and clinical circumstances.
This also includes educational content and notifications (visitor restrictions, live updates, social distancing practices, etc.) on digital signage locations in public areas throughout hospitals. That content can be delivered in notifications or in response to Real-Time Location System (RTLS) triggers (for example, if a clinician enters the room, the patient’s TV will display hand washing reminders).
RTLS integration can also track and report staff entries into patient rooms so hospital leaders have real-time data about potential exposures, isolation violations, or interactions with non-approved staff. Interactive surveys with branch logic can help guide patients to provide vital feedback and report any hand hygiene breaches. Digital meal ordering, service requests, and virtual visits decrease human-to-human contact while helping patients get the food, care, services, and items they need. Live streaming (either soothing content like an aquarium or information sources) can also provide distraction therapy and education for patients in isolation.
To prevent hospitals from being overwhelmed, states should focus on preventing the spread of COVID-19 at high-risk sites, such as nursing homes, and in high-risk localities, the COVID-19 Policy Alliance—a group of experts brought together by two professors at the MIT Sloan School of Management—said in a presentation released today.
The Alliance also put online a set of data analytic tools to enable states to identify the highest risk facilities and localities—those with clusters of individuals over 65 or with relevant health issues.
The Alliance analysis indicates that one of the factors possibly leading to the high fatality rate in Italy was that sick people from areas with concentrations of high-risk individuals overwhelmed hospitals, creating a domino effect that led to skyrocketing death rates. The Alliance has developed tools to identify institutions and counties in every state in the U.S. that have the same characteristics as the points in Italy that put its health care system into a tailspin.
For example, the data tools not only show where nursing homes are and how many people reside in them, but show which nursing homes have had the most problems previously with infections. For counties, the tools show not only areas with high numbers of elderly, but also those with high numbers of individuals of all ages suffering from diabetes, obesity and other conditions that create COVID-19 risk.
A 15-minute webinar describing the Alliance’s tools and recommendations for U.S. federal, state and local policymakers is here. The webinar expands on a slide deck that lays out the analysis and guidance.
The COVID-19 Policy Alliance was launched on March 11 by Professors Simon Johnson, the Ronald A. Kurtz Professor of Entrepreneurship, and Retsef Levi, the J. Spencer Standish Professor of Operations Management. They pulled together a team of experts from across MIT and elsewhere to analyze the available data on the pandemic. The tools will be updated as more data and analysis are available.
Levi said, “We want to help states make data-based decisions that can save lives. Focusing on the sites and areas that are most likely to lead hospitals to crash is key.”
Johnson said, “Hospitals are a critical line of defense in the ongoing battle against COVID-19. We must focus now on preventing our world-renowned hospital systems from collapsing.”



 Dimensional Insight, maker of
Dimensional Insight, maker of 
 To prevent hospitals from being overwhelmed, states should focus on preventing the spread of COVID-19 at high-risk sites, such as nursing homes, and in high-risk localities, the COVID-19 Policy Alliance—a group of experts brought together by two professors at the MIT Sloan School of Management—said in a presentation released today.
To prevent hospitals from being overwhelmed, states should focus on preventing the spread of COVID-19 at high-risk sites, such as nursing homes, and in high-risk localities, the COVID-19 Policy Alliance—a group of experts brought together by two professors at the MIT Sloan School of Management—said in a presentation released today.