By Don Rucker, MD, chief strategy officer, 1up Health
Medicare Advantage is a capitated health plan and the government, which pays for the plan, needs massive amounts of performance data to ensure that plans do right by patients and don’t scrimp on care. With capitation’s pre-determined payment rates, there is an incentive to do less.
The main tool CMS has to monitor performance is the Star Ratings system (though there are lots of other regs to be sure with this as a goal). The data needed to optimize Star Ratings is what fuels the revenue cycle stack in MA plans. In 2025, health plans must
How do these MA payment policies force a rethink about data and technology?
Star Ratings measures of clinical and customer plan performance are reported, then scored and rolled up into overall scores by CMS. These are used to set MA plan, bonuses, other payments and are also reported to patients when they are choosing a plan. This incents two large patterns of behavior – one is to get the underlying data to show performance and the other is to improve that performance. Historically, quality measurement has involved lots of manual steps and even today some data is based on chart pulls and having humans read EMR computer screens. The modern world, a decade of EMR incentives, and modern APIs provide starkly different options to get and improve plan performance data.
Are classic claims dataflows enough or will payers need rich clinical data to succeed?
Not surprisingly, most of the measures deal directly with clinical performance. Today much of Star Ratings scoring is based on claims data – increasingly the winners will use clinical data both to measure performance and to improve performance. It is important to understand the scores are relative – if a plan uses more clinical data and gets a better score that means the plans that don’t use clinical data are more likely to get a lower score. Economists describe this as a “zero-sum game.”
How can plans think about getting clinical data?
Obviously clinical data is captured and stored in EMRs. Certified EMRs are now required to have both patient access APIs as well as Bulk FHIR APIs. Bulk FHIR APIs allow the US Clinical Data for Interoperability (USCDI) to be obtained by the payer from the provider EMR in one swoop if the provider and the payer can reach a satisfactory agreement to share this data in their network contract.
Is getting clinical data enough?
No. It is not just about documenting today’s clinical performance. While that is a large step, the key differentiator will be doing something to improve that performance.
What does a modern digital strategy look like?
A modern digital strategy, whether it is a merchant like Amazon, a service provider like a bank or airline, or a media company, relies on easy access to websites via smartphones and targeted outreach via messaging or email timed to optimize success. For payers that means thinking about what to “say” to patients and providers and how to “hear” from patient and provider feedback, device monitoring data, and clinical data. That is what APIs enable.
Anyone who is interested in signing up for Medicare has many decisions to make, including which type of insurance plan to go with to the type of physicians that they are on the plan. Those living in Florida for example can register a Florida LLC, same with other localities based on existing regulations. But one decision that is particularly important is between using Medicare Advantage plans or going with the more traditional approach to insurance, called Medicare Part A and Part B.
Medicare Part A and Part B
Many people are choosing to stay on their current health plan, called Medicare Part A. The benefits are similar to those of Medicare Part B, except that there is no co-payment required and there are no annual limits on how much you can spend. These plans are also known as Parts A and B. While some doctors agree with the advantages of this type of insurance, other physicians and hospitals are opposed to the use of these plans.
Medigap
Those who are choosing a different type of Medicare coverage are often opting for Medigap, which means that they have an additional deductible, which is why they pay more out-of-pocket. Most people think that if they have a large hospital bill, they will not be able to afford the Medigap premium, so they use Part A instead. However, those with medical conditions that require higher doses of medication, such as heart conditions, kidney diseases or cancers, may be able to qualify for Medigap as a supplement to the original Medicare plan.
After the enactment of the Affordable Care Act, insurers had to cut down on the “cherry-picking” of members and not provide insurance to just low-risk individuals. To some extent, the scope for earning high-profit margins had decreased for health insurance companies. This rule created an imperative for them to look for ways to curb expenses in other ways.
As a result, influential insurers came up with an innovative idea to merge with their contemporaries. Mergers and acquisitions reduce the competition and empower payers to negotiate better with the providers.
However, a lot of Medicare Advantage (MA) markets are served by just one or a small number of insurers and the competition is already bleak. If the few existing insurers also lobby to negotiate contracts, the providers wouldn’t stand a chance to get a decent deal.
US healthcare dynamics are already far from ideal with costs soaring high and quality parameters below most developing nations. The lopsided power play between providers and payers can exacerbate the existing healthcare problems.
To prevent this, the government is making it a point to put brakes on major insurance mergers and acquisitions. At the beginning of 2017 U.S. District John D. Bates ruled against Aetna’s acquisition of Humana. Along with that, the Anthem–Cigna merger was also stopped from going through. It seems like it’s time for payers to think beyond this strategy of creating an oligopoly. It also means that insurers have to compete with each other instead of relying on their collective clout.
Gaining an edge over competitors with improved star ratings
Now that there is no way for insurers to earn strong profits other than by capturing increased market share, they need to look for ways to increase the number of enrollments. For MA plans, their best shot to grow their member enrollments is by achieving credible star ratings. Medicare’s Star Rating system was developed to provide Medicare beneficiaries some concrete insights about a plan’s performance. Every year, CMS evaluates the performance of each MA Plan on quality and cost measures and rates them on a scale of one to five stars. The more stars a plan gets, the more appealing it appears to the beneficiaries, which leads to increased enrollments.
Every health plan aims to achieve maximum operational and cost efficiency and tries to create lucrative offerings for the members. However, unless they are able to do it better than other health plans, their efforts will not bear fruit. The first step to improving their Star ratings is to assess the performance measures of other health plans.
Evaluating the performance of MA plans over the last few years
In 2011, only 24 percent out of all MA Plans got 4+ Star Ratings. By 2018, this figure grew almost by a whopping 50 percent. In a bid to perform better, the health plans brought remarkable changes in their performance. As a result, member enrollments also increased by 17 percent in this tenure.
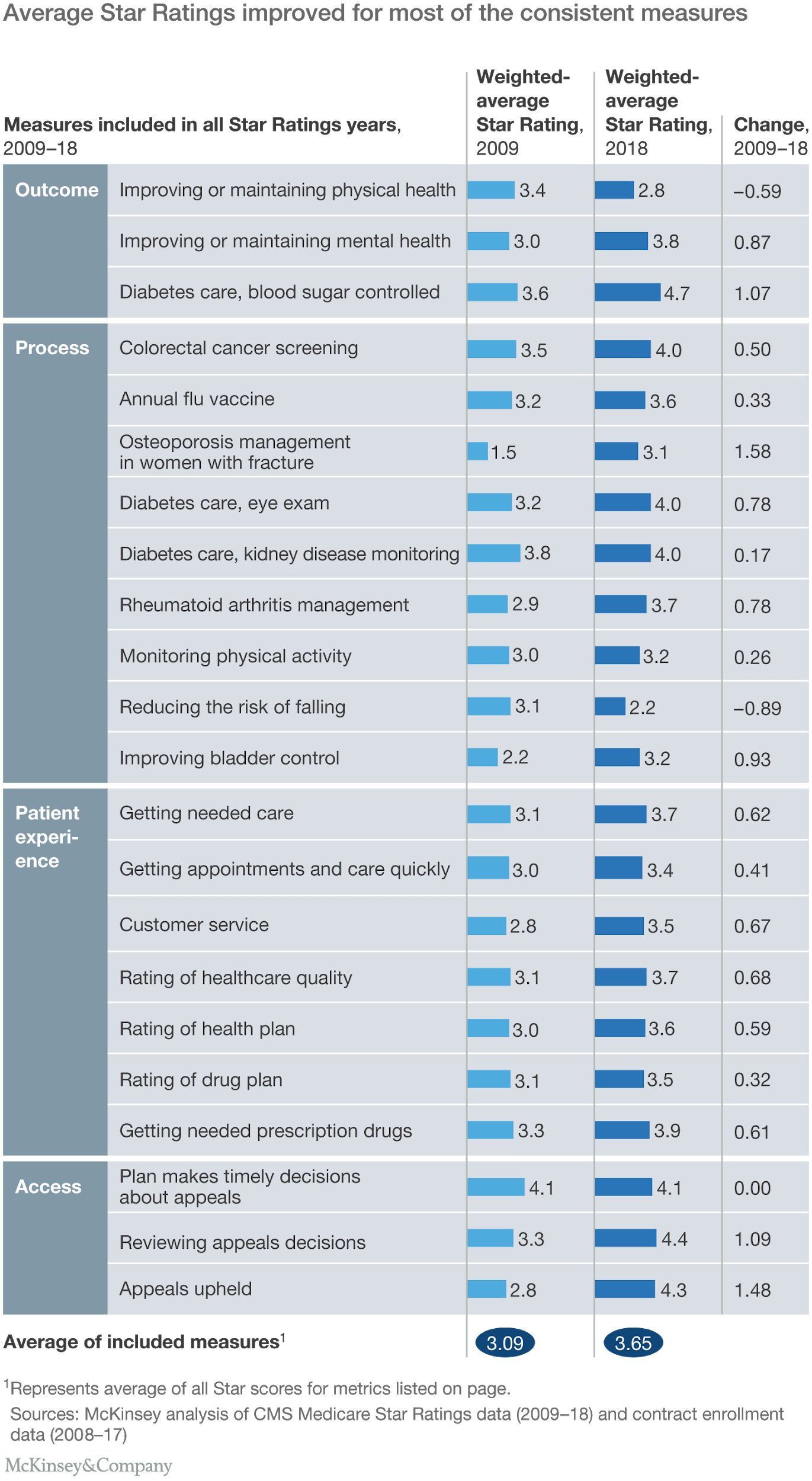
Since the inception of the Medicare Advantage, some measures were modified. However, there were 22 measures that remained consistent between 2009 and 2018. On calculating the average Star ratings of each measure, it was revealed that the average Star ratings had improved by 0.56. The average outcome measures had improved by 0.45 stars, the process measures by 0.49 stars, the patient experience measures by 0.55 Stars and the access measures by 1.12 stars.
Overall, most of the measures showed some improvement. Since 73 percent of the health plans have ratings above 4 Stars, it can be established anything below this can gravely impact the number of member enrollments. On top of that, to match the average performance scores of other health plans, health plans have to earn an average of at least 3.5 Stars.
Creating strategies to perform better than other health plans
An overarching picture of how all the MA plans in the country are performing can be helpful in revealing the measures you need to work on. However, understanding the area-specific operational nitty-gritty is important to find out what steps you need to take to improve the performance of your health plan.
Comparing your plan with top-performing health plans in your area and diving deeper into their measures can unveil what they are doing to perform better than others. This information can be instrumental in devising winning strategies to score star ratings that are better or at the very least at par with other high-performance plans.
In a comment letter submitted to the Centers for Medicare & Medicaid Services (CMS), America’s Physician Groups (APG) applauded the Agency for its work to help strengthen and protect Medicare Advantage (MA) on behalf of the millions of beneficiaries it serves while also noting specific areas of concern with the recently released MA 2020 Advance Notice and Call Letter.
Don Crane
“MA it is a critical component in transforming our nation’s healthcare system from volume to value-based,” said Don Crane, APG president and CEO. “Numerous studies show that despite a higher proportion of clinical and social risk factors, MA beneficiaries have better health outcomes than their peers in traditional Medicare. A strong rate notice is central to supporting this important program and improving our nation’s healthcare system overall.”
APG applauded the Agency’s work to expand supplemental benefits in MA and better address the opioid crisis through certain targeted services and cost-sharing reductions, but expressed concern with the rate adjustment itself, issues related to MA benchmarking, and the implementation of the transition from the Risk Adjustment Processing System (RAPS) to the Encounter Data System (EDS).
The letter closes by highlighting APG’s support for policies in MA which incent plans and providers to participate in risk-bearing models and called for CMS to extend the 5 percent advanced alternative payment bonus to qualified MA providers as a standalone threshold.
“The 5 percent bonus will level the playing field between providers taking risk in MA and those in traditional Medicare,” said Crane. “This will allow greater opportunities and incentives for risk-contracting in MA and will advance the Medicare delivery system for all seniors.”
Please click here for a copy of APG’s comment letter.
Guest post by Ken Perez, vice president of healthcare policy, Omnicell.
Since the passage of the Patient Protection and Affordable Care Act, most of the health reform activity in the Medicaid arena has primarily been about expansion of coverage. According to the Centers for Medicare and Medicaid Services (CMS), as of February 2015, 70.5 million people—more than one in every five Americans—were enrolled in Medicaid or the Children’s Health Insurance Program (CHIP), which represents an increase of almost 40 percent from the number enrolled at the end of 2009.
However, on May 26, CMS aimed its sights on improving the quality of care delivered by Medicaid, issuing a 653-page proposed rule to “modernize the Medicaid managed care regulations,” which have not been revised in a decade. The proposed rule faces a public comment period that will continue thru July 27.
The changes presented in the proposed rule would align the regulations governing Medicaid managed care with those of other major sources of coverage, including Medicare Advantage (MA) plans and Qualified Health Plans (QHPs), which are offered thru health insurance exchanges (marketplaces). CMS has said that the proposed Medicaid measures will emphasize evaluating health outcomes and the patient experience enrollees have with private plans. In addition, the proposed rule mandates public reporting of information on quality of care, as well as the use of financial incentives to reward Medicaid managed care plans that meet quality measures, a la Medicare Advantage Star Ratings.
CMS’s announcement has been met with mostly favorable responses. “It was about time for the changes” has been a common refrain, with the revisions viewed as a natural, logical progression.
How big is the market that will be impacted by the changes? Per CMS, Medicaid managed care organizations (MCOs) have grown from handling 8 percent of Medicaid beneficiaries in 1992 to about 70 percent of the 70 million Medicaid enrollees today—almost 50 million people. That figure compares with 17.3 million MA enrollees as of January 2015.