By Aaron Perreira, director of integrated marketing, Kareo.
Aaron Perreira
A nationwide survey conducted by Kareo reveals an interesting fact for everyone involved in healthcare technology. One of the primary sources from which independent medical practices get advice and information on adoption of new technology is their billing companies.
Independent medical practices remain the primary healthcare delivery system for patients in the U.S. Physician-owned practices see 990.8 million visits, or 3.1 visits per person in the U.S. each year. In contrast, hospital outpatient visits number 125.7 million per year, or .4 visits per person. At the same time, these independent practices – small businesses in most cases – are greatly impacted by the rapidly changing healthcare arena.
Regulatory changes, technology infrastructure demands and increasingly large administrative burdens have put pressure on independent practices in recent years, and they do not have the resources or economies of scale that larger hospital practices have to address them. Experts agree that the primary hope for independent practices thriving efficiently and cost effectively in the emerging healthcare landscape depends upon the effective integration of technology.
One of the steps many independent practices take to help alleviate some of their administrative burden is the outsourcing of billing. Nearly one-third (28 percent) of physicians and medical practitioners who do not currently outsource medical billing indicated that they plan to do so over the next two years. As a result, medical billing companies expect an average revenue growth of 12 percent during 2019 as utilization of outsourced billing by independent medical practices continues to increase. Of course, the primary service billing companies bring to practices is – billing.
The survey highlights that extensive revenue cycle expertise at the specialty level is a successful strategy for building a billing company to scale. Forty-seven percent of small billing companies specialize in order to differentiate themselves, while 58 percent of medium-sized businesses do. As might be expected, large billing companies tend to diversify across a wider range of medical specialties, responding to the rapid growth (11 percent since 2012) in multi-specialty medical practices.
Billing companies are also becoming specialists in patient collections because of the significant increase in high deductible insurance plans – the average deductible for employer-based plans reached nearly $1,500 in 2018 and the average deductible for individual A?ordable Care Act (ACA) Bronze plans was more than $5,800 in 2018. Of those surveyed, patient balances account for an average of 23 percent of total collections.
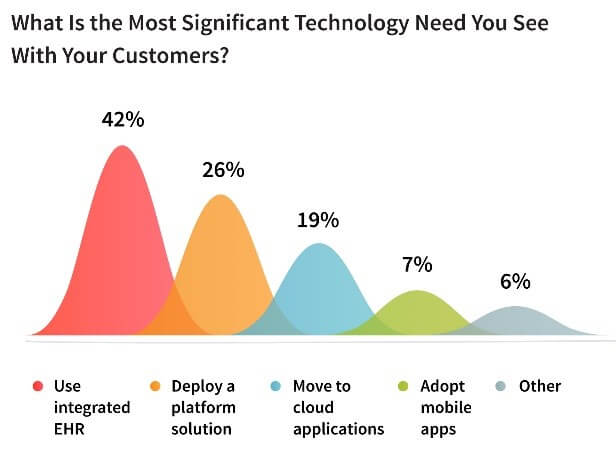
Significantly, billing companies have found an important path to growth in value-added services. Despite the rapid growth of healthcare technology solutions, many smaller practices are still slow to adopt new technology. Billing companies serving small, independent practices have the opportunity to recommend technology to help them improve efficiency, stay competitive in the healthcare delivery marketplace, and run a more profitable practice. Helping medical practices implement and leverage technology is something that 75 percent of billing companies report doing today, with the adoption of integrated EHR and billing software the top area of focus.
With the establishment of value-based payment models that tie reimbursement to the documentation of quality care, many billing companies are seeing the importance of having their clients use a certified EHR that is integrated into their billing platform. The current replacement rate for EHRs is estimated to be as high as 50 percent in the United States, presenting significant opportunity for billing companies to advise on replacement options that will streamline their revenue cycle management process. The survey shows 86 percent of high-growth billing companies are statistically more likely to recommend an EHR solution to their clients that integrates with their billing software/practice management solution.
The Kareo survey points to an interesting chain – the future of American healthcare depends on independent practices. The success of independent practices moving forward depends on technology. And the recent Kareo survey shows that adoption of technology by independent practices depends, to a great extent, on their billing companies.
The healthcare industry has traditionally relied on the pen-and-paper archiving system, creating huge but impractical data libraries. However, the situation is changing in the last couple of decades with the introduction of electronic health records (EHR).
According to the report, more than 80 percent of the US hospitals adopted at least a basic EHR system. It’s a major improvement that drastically changes the way medical practitioners complete their everyday tasks. But what makes EHR systems so powerful? How can they contribute to the overall productivity in the field of medicine?
We will give you the answers to these questions in this article. Keep reading to see how EHR are impacting the healthcare industry.
5 ways EHR changes healthcare
There are many ways EHR is helping healthcare to advance, but some solutions already proved to be very important for the functioning of the medical staff. We made a list of the five most important improvements here:
Speed and productivity
The first way digital health records are influencing the healthcare industry is obvious: they help the system become better and more productive. Medical staff no longer has to write things down. Instead, all entries are just a few clicks away, so the whole process becomes faster than ever before. This gives doctors and nurses more time to do what they are trained to do – help patients to get better.
Improved treatment
The second way EHR is changing medicine is probably the most important. Namely, patients get an enhanced treatment due to the precision and transparency of medical records. For instance, a doctor can instantly see previous health problems of a patient and determine whether this person is allergic to certain drugs or substances.
By Gevik Nalbandian, vice president of software development, NextGate
Gevik Nalbandian
If you wanted a clear snapshot of the progress we’ve made—or rather, haven’t made—in patient data sharing and exchange, look no further than a new report from the American Hospital Association (AHA) and six other national hospital associations—America’s Essential Hospitals, Association of American Medical Colleges, Catholic Health Association of the United States, Children’s Hospital Association, Federation of American Hospitals and the National Association for Behavioral Healthcare.
Urging all stakeholders to “unite in accelerating interoperability,” the report, released January 22, is a grass roots effort to get hospitals, EHR vendors, consumers, health information exchanges (HIEs), government and medical device companies to come to the table, play their respective roles, and make full interoperability a reality.
The benefits of interoperability are obvious: better care coordination, improved patient safety and care quality, reduced costs, increased efficiencies and the conduit to population health. Interoperability is also increasingly a legal requirement and prerequisite for reimbursement.
So why has healthcare’s goal of industry-wide interoperability remained so elusive?
By B.J. Boyle, vice president of product management, PointClickCare.
B.J. Boyle
Interoperability, as it was envisioned, should be built on transparency and connectivity, allowing a patient’s critical health information to be easily accessible, regardless of where treatment is being administered. By creating an infrastructure that supports the sharing of patient data along the care continuum, hospitals, skilled nursing facilities (SNF) and long-term post-acute care (LTPAC) facilities can offer the best care possible. As a result, organizations that participate in interoperability best practices are positioned to become preferred providers.
Unfortunately, interoperability is still a work in progress for many organizations. While more than 95 percent of hospitals and 90 percent of office-based physicians are now utilizing electronic health record (EHR) platforms, many struggle with — or have reservations around — sharing information outside of their facility. As such, silos represent a great barrier to realizing a fully implemented state of interoperability.
The current data gap can drastically impact care. For example, a patient experiences a serious medical incident — such as a fall or stroke — and arrives at the hospital where staff may not have access to existing patient data which could inform the best delivery of care. Or perhaps they’re able to access that data, but not right away. Care is now delayed, which can be additionally concerning depending on the time-sensitivity of the patient’s condition.
Taking this example a step further, let’s explore what happens after care at the hospital has concluded. The patient requires rehabilitation, and a continuation of care document (CCD) is issued to a post-acute care facility. From there, the patient’s information is transferred by less-than-foolproof methods such as fax, for example. A glitch as simple as a jammed paper feed could prevent critical information from reaching the appropriate caregiver.
As value-based care and payment-care models are moving toward the forefront, blind handoffs of patient information are no longer viable, as they drastically increase the financial risks hospitals and payer groups are subject to — not to mention the clear detriment the system has on delivery of care.
Closing the gap
The larger question is how does the industry get from Point A to Point B? The easy answer is to liberate the data through a cloud-based infrastructure that supports an efficient, easy-to-access data exchange between all caregivers. An integrated solution would connect stakeholders across the care continuum, providing accurate insights when needed, eliminating data silos between care partners, and enabling more confident decision-making.
These systems would promote:
Optimized transitions: Data needs to travel with the patient — or before movement — discretely across all systems.
Patient visibility: Data should reflect the most current ADT information, identifying and sharing where a patient is and from where they’ve been discharged.
Central view of LTPAC patients: This facility-agnostic feature should offer automated updates of a patient’s functional progress.
Ongoing status and monitoring: Maintaining continued care is facilitated through alerts and notifications to caregivers regarding any change to their status or well-being and meaningful feedback on care pathway progress.
Facility performance: Beyond understanding a patient’s status, it’s also helpful to understand how facilities in and out of their PPN have performed.
Overcoming concerns
The concept of interoperability, in some ways, seems contradictory to traditional best practices. Healthcare organizations are charged with protecting patient data at all costs, and the idea of sharing data in a way that opens access to a wider group of stakeholders could give pause. Regulatory infractions for data loss in the healthcare industry can be steep, and the number of well-publicized data breaches in recent years reinforces how valuable health records are to both the organizations who keep them and those who try to steal them.
So, it should go without saying that an EHR “superhighway” must be developed with security in its DNA, taking stringent regulatory requirements into account. The good news is that the newest breed of information exchange platforms is being built with security roles in mind, drastically reducing the possibility of data loss.
If you ask doctors, you’ll hear that electronic health records (EHR) have been both the best thing and worst thing to happen to medicine in the past 40 years. Having real-time information at your fingertips is an incredible advancement, but it’s only helpful if you can see what you need to diagnose and treat your patient. Healthcare providers consistently state their frustration with the lack of consistent, accurate data within the EHR system.
Without accurate data in the patient’s chart, doctors struggle to provide accurate and appropriate care. That’s why clinics and hospitals need to go the extra mile and customize their records in the following ways:
Invest in consulting to configure software
It’s too much to ask of our healthcare providers for them to become IT and software experts. Accessing records of earlier care and making accurate diagnoses is dependent on doctors and providers’ ability to input and extract relevant information quickly.
Even a lively family physician practice needs assistance to set up and configure an electronic healthcare record system. Even with technical staff, it’s unrealistic to expect them to configure and customize a highly complex software system to suit a unique workflow. As organizations upgrade or adopt new technology, they are relying on artificial intelligence or a technical sales support representative to migrate data.
Data is only as good as the input
Without expert configuration and data migration, the accuracy of the data is in question. Patient records need to be correct, and it needs to appear in the right place in the record. Relying on a software program to migrate data accurately may preserve your data, but if it doesn’t populate the proper fields, it’s not useful.
Efficiency is key
With only 20 minutes to see each patient, the data needs to be more than accessible. Many small offices find it cost prohibitive to fully take advantage of the software system’s features and discover it’s even more challenging to configure and customize the software to meet its full potential. Although the cost is a prominent factor, the value of a properly configured and deployed EHR is priceless.
Hire a consultant
Setting up an electronic health record is a complex endeavor. Innovative software design makes it possible to customize fields, provide reporting, and give alerts. Used efficiently, an EHR can help doctors reach conclusions more quickly and show information in a way that leads to faster diagnoses.
If the EHR isn’t configured efficiently, or if the data isn’t captured in a way that providers can access and leverage it to make smart clinical decisions, it becomes more of a roadblock than a powerful tool. Apathetic software users create inaccurate or missing data.
By Inga Shugalo, healthcare industry analyst, Itransition.
Inga Shugalo
Following the wind of change, we find that healthcare is on the way to transferring most of its processes to the cloud. According to IDC, hospitals now tend to prefer keeping custom medical software from EHRs to AI and data analytics on cloud servers instead of in-house management.
With more providers investing in scalability and cost-efficiency of cloud solutions, the recent research forecasts the global healthcare cloud computing market to reach $35 billion by 2022 at 11.6 percent CAGR.
Currently, the cloudification develops in two complementary directions.
Some providers only test the waters going for a new cloud solution, for example, a mobile app to support chronic disease management. Others consider migrating their already existing architecture elements to the cloud to enable seamless synchronization between different system parts, create new team collaboration practices, or save time and money on the infrastructure maintenance.
Since cloud migration is a complex process requiring substantial planning and good timing, we’ve decided to cover the initial steps of a smooth transition to the cloud.
Assessing the infrastructure
First things first, there is a good chance you don’t need to migrate the full infrastructure and can better manage your investments by injecting them into strategic areas only. Start with considering your as-is situation and pinpointing the architecture components with the potential to impact the business evolution via new or improved services.
Additionally, take into account the possible technology and business constraints, upcoming updates, integration and compatibility requirements for the solutions, as well as the need for a substantial redesign before starting the cloud migration.
It can turn out that some big data archives that aren’t used frequently can stay on-premise, and some applications will serve providers better from the cloud due to increased robustness and security for the regular multi-user access.
In this case, an organization can choose to go for the hybrid environment, decreasing the load on in-house servers and adding up more flexibility to the picked system elements.
Self-check: What are our migration goals?
Answering this question, you will be able to determine the priority elements for migration to the cloud by determining the most pressing needs, such as everyday workflows, equipment management, or disaster recovery.
While thinking about the goals, review all parts of the infrastructure, including business and clinical applications, such as EHR, LIS, PACS, and RIS, assigning them to one of the following categories:
First to be migrated
Future migration projects
Unable/unneeded to migrate
With such a clear prioritization, it will be easier to assemble a migration roadmap that will guide the project scope creation, design, and implementation processes.
Drafting a migration strategy
After your priorities are all set, it is time to create a migration strategy based on applications and data to be transferred to the cloud. You can either pick one of the approaches or mix and match them depending on particular infrastructure elements.
There are many uses of information technology in healthcare. In the previous years, these implementations have developed more than anyone could anticipate. They boost efficiency, improve the quality of care and security and control costs. These advancements have created many benefits for the patients and medical facilities in both the public and the private sector. When asked, experts say that these are some of the biggest health IT issues that should be considered:
Interoperability
Interoperability, when it comes to healthcare is one of the processes that make it easier for medical services to share information on patients. It makes the healthcare more efficient — it prevents doing the same tests multiple times on one patient and it helps specialists communicate quickly through the system.
This is why it’s so crucial that this technology continues advancing and moving further while making the job of doctors all over the world as simple and as focused on the problem as possible.
Security
Of course, with so much data which exists in healthcare field, security of that data is one of the top priorities. In recent years we have come across so many examples of how not to handle patient data but now that we are dealing with population Healthcare, we need to be even more careful. That’s why cyber security of the data became an imperative at so many companies.
“Security is something that you should definitely keep an eye on. Whenever you see that there is a new update, make sure that your healthcare organization has it. People are getting more and more skilled at hacking and obtaining data that this has to be a priority,” said Gina Petrelli, a data analyst from OriginWritings and WriteMyX
Big Data
Because there is such a shortage of trained medical personnel in the world, big data will have to become the main source for point-of-care information. This can improve the current state of health in certain groups as well as establish customization so that every technology can be unique to each culture. It will also help develop safer and more efficient systems across the world.
Big data means that there are many sources and a lot of data to be taken from them — medical professionals will have the kind of information that they usually can’t easily get.
Investments
Over the years, there have been some big investments made towards the healthcare technology industry. However, those investments are noticeable now more than ever — technologies are advancing fast and this progress is visible in many areas.
Investments in healthcare information technology has mostly been aimed at technologies that improve efficiency, technology that supports decision making and personalized medicine, technology that empowers patients, technology that protects against cyber attacks and technology that enables remote health monitoring.
Why most investments are made towards these areas is understandable — they contribute to the overall health and safety of populations.
Improvements of EHR
Electronic health records are something that is already in place and has been for some time now. While there are many benefits to this, it can sometimes be a nuisance and a burden to medical professionals. They are often not inter-operable and that causes a lot headaches to doctors across the world. Any technology that allows for easier use and interoperability is going to be well-accepted.
“While we’ve had these technologies for years now, you’ll have to notice that they caused many troubles – security, operating, transitioning from paper to digital. New improvements could change that,” said Dennis Marks, a communication manager at 1Day2Write.
Telemedicine
Growth of telemedicine has been steady over the years but the growth will speed up in the future years. This will enable doctors to examine patients using wearables and use that data to assist them in diagnostics, management and prevention later. This is all thanks to MACRA, value-based demands placed upon the providers and so on.
By Poornima Venkatesan, senior consultant, Virtusa.
Poornima Venkatesan
In today’s value-based care environment, patient engagement is a vital key to success in clinical outcomes. This is especially true for chronic diseases such as arthritis, where continuous care is necessary because of the disease’s physical, emotional and economic impact on patients. Although the advent of specialty drugs in the past decade has made disease control possible, clinicians still face challenges in patient care because patients’ preferences about therapy aren’t often considered.
Understanding patient goals and expectations
While a clinician’s goal is to achieve remission, a patient’s goal could be clinical or nonclinical and varies depending on their individual characteristics and demographics.
Patients from low-income countries such as Morocco expect access to primary care (never mind rheumatologists), support services and education about the disease. The high expenses related to rheumatoid arthritis (RA) in such countries result in poor treatment compliance, school absenteeism in children and deterioration in quality of life. Comparatively, even with excellent health insurance systems in the United States, one in six adults with RA reduce their medication use because of high out-of-pocket costs. Most patients expect cost-effective care. In wealthier countries like the United Kingdom, patients expect increased social connectedness and family support.
Elderly patients expect reduced pain, fatigue and side effects, whereas young adults expect independence and normalcy from their treatments. Women, who are most affected by RA, might expect a lesser impact on family life and childrearing.
If such multidimensional expectations are not met, patients tend to discontinue their treatment. As new biologics and non-biological complex drugs (NBCDs) are developed, patient adherence is essential in determining both therapeutic and potential adverse effects. Studies reveal that frustration towards the method of drug administration (like self-injection) also impacts adherence. In the U.S alone, the total cost of non-adherence is estimated between $100 billion and $289 billion annually.
Therefore, it is important for the patient and the physician to trust each other and have open discussions about treatment strategies and expectations to ensure better alignment and cooperation.
Measuring patient engagement
The first step towards patient engagement is awareness of their current engagement levels. The patient activation measure (PAM) tool is helpful here. PAM measures the attitude and knowledge of patients about the disease and treatments. Studies have proven that highly activated patients have better outcomes via increased medication adherence, resulting in lower healthcare costs through fewer ED visits, hospital admissions and re-admissions. By continuously monitoring activation levels, providers can measure sustained changes in patient behavior and personalize their care programs.
We can also measure engagement levels by taking advantage of data. Data derived from direct [electronic health records (EHR), claims] and indirect sources (wearables) provide a holistic view of an individual patient. Simple analytics applied to population data can predict patient behavior. For example, analytics can help providers know which patients are likely to miss their appointments, which patients will fill their prescriptions on time, and so on. Detailed patient-based data could also lead to better and more accurate diagnoses and treatments.

 Significantly, billing companies have found an important path to growth in value-added services. Despite the rapid growth of healthcare technology solutions, many smaller practices are still slow to adopt new technology. Billing companies serving small, independent practices have the opportunity to recommend technology to help them improve efficiency, stay competitive in the healthcare delivery marketplace, and run a more profitable practice. Helping medical practices implement and leverage technology is something that 75 percent of billing companies report doing today, with the adoption of integrated EHR and billing software the top area of focus.
Significantly, billing companies have found an important path to growth in value-added services. Despite the rapid growth of healthcare technology solutions, many smaller practices are still slow to adopt new technology. Billing companies serving small, independent practices have the opportunity to recommend technology to help them improve efficiency, stay competitive in the healthcare delivery marketplace, and run a more profitable practice. Helping medical practices implement and leverage technology is something that 75 percent of billing companies report doing today, with the adoption of integrated EHR and billing software the top area of focus.


 If you ask doctors, you’ll hear that electronic health records (EHR) have been both the best thing and worst thing to happen to medicine in the past 40 years. Having real-time information at your fingertips is an incredible advancement, but it’s only helpful if you can see what you need to diagnose and treat your patient. Healthcare providers consistently state their frustration with the lack of consistent, accurate data within the EHR system.
If you ask doctors, you’ll hear that electronic health records (EHR) have been both the best thing and worst thing to happen to medicine in the past 40 years. Having real-time information at your fingertips is an incredible advancement, but it’s only helpful if you can see what you need to diagnose and treat your patient. Healthcare providers consistently state their frustration with the lack of consistent, accurate data within the EHR system.
